2025: Volume 6, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFAortoduodenal Fistula with Ruptured Aortic Aneurysm: A Challenging Case with Fatal Outcome
Reet Ramani, Syed Shahrukh Parvez, Aimen Noor ul Ain, Umer Shahid, Abuzar Hussain, Muhammad Yaqoob*
Ziauddin Medical College, Ziauddin University, Karachi, Pakistan
*Corresponding author: Muhammad Yaqoob, Ziauddin Medical College, Ziauddin University, 4/B Shahrah-e-Ghalib Rd, Block 6 Clifton, Karachi, Karachi City, Sindh 75000, Pakistan, Phone: 03022018960, ORCID: 0009-0008-4129-286X, E-mail: [email protected]
Received Date: May 20, 2025
Publication Date: June 19, 2025
Citation: Ramani R, et al. (2025). Aortoduodenal Fistula with Ruptured Aortic Aneurysm: A Challenging Case with Fatal Outcome. Clin Res. 6(1):29.
Copyright: Ramani R, et al. © (2025).
ABSTRACT
Aortoenteric fistulas (AEF) exist as an uncommon, lethal gastrointestinal bleeding, which can start with a hidden bleeding episode that leads to severe hemorrhage. The patient is a 65-year-old male who had no reported medical conditions before developing severe gastrointestinal bleeding because of an aortoduodenal fistula associated with his infrarenal aortic aneurysm. Multiple endoscopy procedures failed to detect the bleeding source, which led to the final diagnosis from CT mesenteric angiography. The patient underwent emergency open surgery to fix the condition, but died due to multi-organ failure. The presented case illustrates the challenging nature of AEF diagnosis, along with the necessity for prompt treatment and unfavorable clinical outcomes. Quick identification of medical indicators combined with proper imaging methods must be followed by multidisciplinary team coordination to achieve better outcomes.
Keywords: Aortoenteric Fistula, Aortoduodenal Fistula, Gastrointestinal Bleeding, CT Angiography, Herald Bleed, Vascular Emergency
INTRODUCTION
Aortoenteric fistula (AEF) exists as a dangerous connection between the aorta and the gastrointestinal system. The two categories of AEFs include primary and secondary types. The spontaneous development of primary aortoenteric fistulas (PAEFs) mostly happens because of atherosclerotic abdominal aortic aneurysms [1]. The development process of secondary aortoenteric fistulas (SAEFs) begins when patients undergo prior aortic surgery or need graft implantation. AEFs appear as the dominant primary fistulas because they affect the third and fourth segments of the duodenum, where the duodenum and aorta exist in proximity in the retroperitoneal space. Primary AEFs rarely occur, but claim all patients do not receive immediate treatment since their mortality rate reaches nearly 100% [2].
Duodenal aneurysm enlargement produces a slow compressive duodenal force that results in tissue necrosis following blood reduction until the bowel wall is jeopardized. Two processes combine their effects to cause the formation of a fistula. These processes include mechanical stress with inflammatory changes [3].
Gastrointestinal bleeding from AEFs demands the utmost recognition by medical staff because standard evaluations may not detect the affliction.
CASE PRESENTATION
The 65-year-old patient without any recorded past medical conditions, visited the emergency department because of sustained abdominal pain and then developed the symptoms of melena and hematemesis. The patient exhibited hypotension (BP 80/50 mmHg) combined with tachycardia (pulse 140 bpm) and hypoxic SpO2 readings of 75% under room air conditions. The laboratory tests showed a severe anemia condition (Hb 5.1 g/dL) together with elevated leukocyte numbers (WBC 17,000/mm³) but a normal platelet count.
The first esophagogastroduodenoscopy (OGD) showed many blood clots in the stomach without identifying any bleeding origin. The gastric ulcer received adrenaline therapy, yet the third and fourth parts of the duodenum remained outside the endoscopic view during a second endoscopy. Sigmoidoscopy was unremarkable. The fluid analysis from the nasogastric tube collected 3.5 liters of bloody material.
The patient maintained uncontrolled blood pressure after receiving 8 units of packed red blood cells and 4 units of fresh frozen plasma. CT mesenteric angiography demonstrated an infrarenal aortic saccular aneurysm at the level of L3-L4 measuring 36.6 x 39.4 mm anteroposterior (AP) and transverse (TR) [Figure 1], which partly contained thrombus and had an enlarged duodenal lumen space due to a suspected aortoenteric fistula near the proximity to the duodenal wall [4].
The aneurysmal neck measured 17.5 mm, as shown in [Figure 2]. The residual aortic lumen measures 16.7x11.8mm in AP x TR dimensions. The body of the aneurysm is closely abutting the third and fourth parts of the duodenum, associated with increasing hyperdensity in the duodenal lumen on the arterial and venous phases, suggestive of aortoenteric fistulous communication.
A surgical exploration through laparotomy showed an 8 mm hole in the anterior aortic wall, accompanied by intestinal perforation in the duodenum. The fistula existed within thick adhesions and a severe state of inflammation. The surgical procedure included free omental patch restoration of the aortic defect, followed by two-layer duodenal repair as well as proximal jejunum serosal tear repair.
Throughout their recovery period, the patient received double inotropic medication support. The patient's condition worsened within 24 hours to show multiorgan failure symptoms along with oliguria amounting to 20 mL during six hours and elevated coagulation markers (INR 3.6) with a platelet count of 48,000/mm³ in addition to severe hepatic damage (ALT 3,250 U/L and AST 10,530 U/L). Rapid kidney damage occurred during the postoperative period (creatinine reached 5.51 mg/dL). The patient received 16 units of PRBC together with 14 units of FFP as well as 10 platelet units before experiencing refractory hypotension that resulted in cardiac arrest on postoperative day 2. Reanimate efforts failed to revive him.
On Day 1, the patient arrived at the emergency department with abdominal pain. First endoscopy and resuscitation were performed in 6 hours. On Day 2, repeat OGD and sigmoidoscopy were done. The diagnosis was confirmed by CT angiography on Day 3, and emergency laparotomy was carried out on the same day. The patient developed postoperative complications and died on the second postoperative Day.
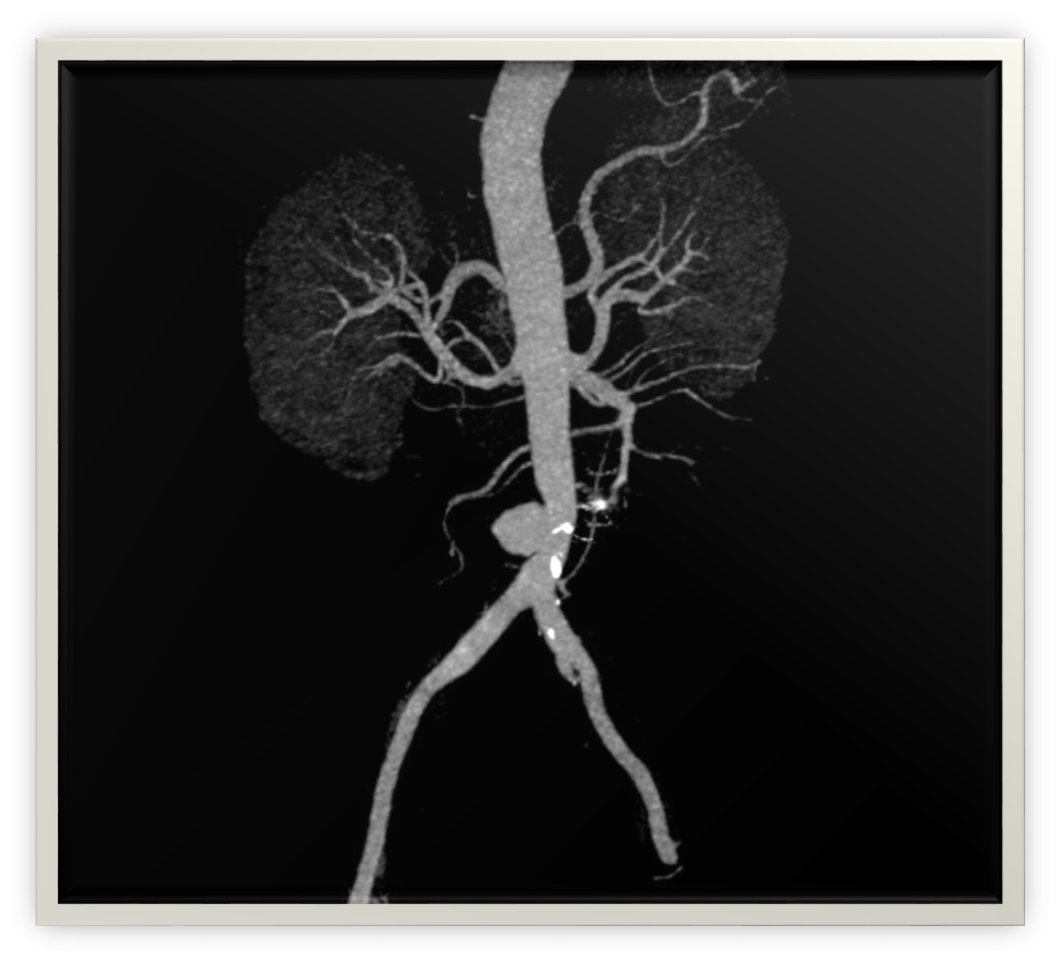
Figure 1. CTA Abdomen/Pelvis.

Figure 2. CT Abdomen.
DISCUSSION
Emergency medical professionals must react rapidly to primary AEFs because these events are life-threatening vascular disasters. The third part of the duodenal segment is at great risk because of its unique fixed position along the infrarenal aorta. Aneurysmal expansion causes chronic mechanical force, which produces a destructive process resulting in fistula development.
Similar pathological mechanisms have been observed in cerebral aneurysms, where hemodynamic stress and chronic inflammation lead to extracellular matrix degradation and vascular wall remodeling, contributing to aneurysm rupture [5].
The bleeding manifestations of primary aortic-duodenal fistulas consist of periodic gastrointestinal bleeding as well as dramatic bleeding events [6]. A herald bleed describes an episodic gastrointestinal bleeding that appears before a full-blown exsanguinating hemorrhage. Medical staff need to maintain constant vigilance because the time interval between heralding bleeding and significant bleeding events is unpredictable.
The hidden location and blood that covers the abnormal fistulae make endoscopy an ineffective method for AEF detection [7]. Several endoscopic gastrointestinal duplications failed to provide a definitive detection of the source. CT mesenteric angiography serves as the preferred diagnostic method since it brings forth both primary and secondary manifestations of fistulization [8].
Healthcare solutions for treating the condition include either open surgical repair (OSR) or endovascular aneurysm repair (EVAR) [9]. Despite being a curative procedure, OSR is associated with high perioperative mortality rates (30%–50 %) due to the extensive nature of the surgery and the critical condition of the patients [10]. Both the aortic and enteric defects received direct surgical treatment during the operation through OSR. EVAR does not remove the underlying infection and is associated with risks of persistent or recurrent infection, graft sepsis, and potential recurrence of the fistula. Consequently, EVAR may serve as a bridge to definitive surgical repair or may require lifelong antibiotic therapy to manage infection risks [11]. While EVAR offers a lower initial surgical risk, its long-term efficacy remains a concern due to the risk of persistent sepsis and rebleeding.
Decreased survival rates postoperatively occur because of sepsis and SIRS (Systemic Inflammatory Response Syndrome) and multiorgan failure, and the lethal combination of coagulopathy together with acidosis and hypothermia [12]. These fatal cardiac arrest conditions evolved from our patient's severe renal failure and liver dysfunction, along with a blood clotting disorder. Emerging management strategies focus on targeted immunomodulation, advanced organ support, and antimicrobial control to improve long-term outcomes in patients undergoing complex vascular repair [13].
The clinical presentation demands that healthcare providers maintain awareness about patients who experience GI bleeding symptoms and aortic disease conditions. A combination of vascular surgeons, gastroenterologists, intensivists, and radiologists must collaborate to help reach optimal treatment results. Intensive care management benefits from the SOFA (Sequential Organ Failure Assessment) score, which helps clinicians predict patient outcomes.
Since the patient was hemodynamically unstable during the procedure, other approaches like damage control surgery (DCS) or an endovascular approach could have been considered. DCS, with its emphasis on controlling rapid hemorrhage and temporizing abdominal closure, would have reduced the significant operative stresses over an extended period, and definitive repair would have been performed once the physiology has been stabilized. Also, endovascular repair, with its limitations in contaminated fields because of the risk of infection, could provide a less invasive bridging procedure in unstable patients. Such methods should be taken into account in future cases with similar critical presentations.
CONCLUSION
Primary aortoduodenal fistulas exist as a very infrequent yet life-threatening condition that requires prompt diagnosis and surgical intervention. Time spent diagnosing primary aortoduodenal fistulas becomes worse due to nonspecific symptoms along with endoscopic diagnostic limitations. Early clinical suspicion, together with CT angiography, should be followed by multidisciplinary approaches as the best means of optimal care. Surgical procedures used for treatment require immediate action, but post-surgical results might be unfavorable due to entire body. The surveillance of AEFs, together with proper diligence toward both patients showing unexplained gastrointestinal bleeding and those with established or potential aortic conditions, proves vital to save lives.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
REFERENCES
- Ho S, Liu B, Loya R, Koury I. (2016). Primary Aortoenteric Fistula: A Rare Case of a Massive Gastrointestinal Bleed. Cureus. 8(9):e766.
- Burks JA Jr, Faries PL, Gravereaux EC, Hollier LH, Marin ML. (2001). Endovascular repair of bleeding aortoenteric fistulas: a 5-year experience. J Vasc Surg. 34(6):1055-1059.
- Oikonomou K, Pfister K, Kasprzak PM, Schierling W, Betz T, Sachsamanis G. (2022). Treatment of Secondary Aortoenteric Fistulas Following AORTIC Aneurysm Repair in a Tertiary Reference Center. J Clin Med. 11(15):4427.
- Hagspiel KD, Turba UC, Bozlar U, Harthun NL, Cherry KJ, Ahmed H, et al. (2007). Diagnosis of aortoenteric fistulas with CT angiography. J Vasc Interv Radiol. 18(4):497-504.
- Chen S, Li Q, Wu H, Krafft PR, Wang Z, Zhang JH. (2014). The harmful effects of subarachnoid hemorrhage on extracerebral organs. Biomed Res Int. 2014:858496.
- Deijen CL, Smulders YM, Coveliers HME, Wisselink W, Rauwerda JA, Hoksbergen AWJ. (2016). The Importance of Early Diagnosis and Treatment of Patients with Aortoenteric Fistulas Presenting with Herald Bleeds. Ann Vasc Surg. 36:28-34.
- Chiche L, Pitre J, Sarfati PO. (1999). In situ repair of a secondary aortoappendiceal fistula with a rifampin-bonded Dacron graft. Ann Vasc Surg. 13(2):225-228.
- Vu QD, Menias CO, Bhalla S, Peterson C, Wang LL, Balfe DM. (2009). Aortoenteric fistulas: CT features and potential mimics. Radiographics. 29(1):197-209.
- Spanos K, Kouvelos G, Karathanos C, Matsagkas M, Giannoukas AD. (2017). Current status of endovascular treatment of aortoenteric fistula. Semin Vasc Surg. 30(2-3):80-84.
- Latz CA, Boitano L, Schwartz S, Swerdlow N, Dansey K, Varkevisser RRB, et al. (2021). Contemporary mortality after emergent open repair of complex abdominal aortic aneurysms. J Vasc Surg. 73(1):39-47.e1.
- Nakajima K, Kato N, Hashimoto T, Chino S, Higashigawa T, Ouchi T, et al. (2018). Treatment of Infected Aneurysm with Combined Endovascular Aneurysm Repair and Abscess Drainage. J Vasc Interv Radiol. 29(2):188-193.
- Erdoes LS. (2006). Endoscopic vein harvest in peripheral vascular surgery. J Vasc Surg. 44(2):417-418.
- Sharma P, Kulkarni AV. (2024). Prevention and treatment of infections in cirrhosis. Clinics in Liver Disease. 28(1):1-14.