2020: Volume 1, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFObesity and Food Addiction: Consumption of High-Fructose Corn Syrup and the Effectiveness of Clinical-Nutritional Management
Rafael Torres-Valadez1,2*, Maria G. Sandoval-Parra2, Eloy A. Zepeda Carrillo1,3*
1Specialized Unit in Research, Development and Innovation in Genomic Medicine, Nayarit Center for Innovation and Technology Transference, Autonomous University of Nayarit, Tepic, Nayarit, Mexico 2Integral Health Academic Unit, Degree in Nutrition, Autonomous University of Nayarit, Tepic, Nayarit, Mexico 3Civil Hospital Dr. Antonio González Guevara, Health Services in Nayarit, Tepic, Nayarit, Mexico
*Corresponding author: Unit specialized in Research, Development and Innovation in Genomic Medicine, Nayarit Center for Innovation and Technology Transfer, Autonomous University of Nayarit, Av. Emilio M. Gonzalez S/N, Col. Ciudad Industrial, Tepic, 63173, Nayarit, Mexico, E-mail: [email protected]; Tel: +52-331-252-3644. Received: December 14, 2019 Published: August 26, 2020
ABSTRACT
Over time, food has undergone modifications to become an unhealthy diet. Currently, the consumption of processed foods with a high content of simple sugars and saturated fats is preferred, making the food a health risk. This situation has increased obesity rates becoming a serious problem worldwide. The constant consumption of foods enriched with high-fructose corn syrup exerts a direct effect on the dopaminergic mesolimbic system, estimulate the synthesis of dopamine causing a sensation of pleasure. Continued use of these foods establishes the process of food addiction, which causes neuroadaptive changes and increased reactive tolerance. This causes overeating even knowing the health consequences. The uncontrollable weight gain highlights the need that obesity to be considered as a condition derived from an addictive process. Moreover, the constant failure of clinical-nutritional treatments in the obese patient is related to food addiction. Continuous contact with processed foods causes an addictive reminder, which favors the patient to regain lost weight. This is why the need to modify the approach to obesity, implement specialized treatments involving a multidisciplinary team. In this way, it will be possible to directly influence the problem of obesity, which is a direct cause of the main pathologies that affect today's world society.
Keywords: Obesity; Food Addiction; High-Fructose Corn Syrup; Cerebral Reward System; Dopamine; Addictive Process
INTRODUCTION
Obesity and its metabolic disorders have become in serious public health problems worldwide [1]. The uncontrollable increase in obesity rates has caused health experts to estimate that more than 1.9 billion adults worldwide have excess body weight [2]. The current diet of majority of the countries is characterized by an excessive consumption of processed food rich in high-fructose corn syrup, as well as low intakes of vegetables and fruits [3]. These food trends have increased the amount of simple carbohydrates in the diet, with which individuals can develop a compulsive consumption of these foods, creating an addictive behavior [4].
Several studies have been document addictive behavior to food [5]. Foods high in sugar, fat and salt have similar effects on the brain to some stimulating substances such as cocaine and nicotine. In this sense, people with obesity tend to select foods with high energy density, compared with non-obese people [4]. The feeding based on hypercaloric foods, causes the activation of the neurotransmitters of the brain reward system resulting in a feeling of pleasure. This sensation will be repeated constantly to experience pleasure again, which will lead to overeating by developing addictive behaviors [6].
It has been shown that a lower availability of the type 2 dopaminergic receptor (DRD2) influences the consumption of diets high in sugar, altering the neurocircuit of pleasure [7]. In addition, compulsive and obese consumers have a reduction in dopaminergic activity, poor inhibitory control and reduced sensitivity to pleasure. This disturbance in the brain reward system, specifically, that characterized by a lower density of the type 2 dopaminergic receptor (DRD2) causes in people an excessive increase in the body mass index until reaching obesity [8].
Food addiction causes a difficult attachment of the obese patient to any type of conventional clinical-nutritional treatment. This situation is closely related to direct contact with foods rich in high-fructose corn syrup, which stimulates the urge to consume these foods, leading to weight gain [9]. Thus, the aim of this work is to describe the importance of the additive process in the development of obesity and the contribution of the consumption of high-fructose corn syrup in food addiction. We conclude with an analysis on the causes of detachment of the obese patient to clinical-nutritional treatment and the aspects that should be considered to increase the effectiveness of these therapies.
Diet Development
Historical Evolution of the Feeding
Food, throughout its history, has undergone drastic changes, defining very specific stages, from primitive times to modern life. In the case of ancient civilizations, their diet was quite natural and was limited to the bioavailability of food in the region [10,11]. In the American continent, the maize “Zea mays” was the basis of the diet, which elaborated dishes such as “tortillas”, “tamales” and “atole” [12]. Besides, they included other types of foods such as beans, onion, avocado, chili and tomato; also fruits such as “tejocote” (Crataegus Mexicana), prickly pear, guava and pineapple. The Animal protein consumption was limited; it was possible to obtain meat of turkey and fish. Despite the limited amount of food, it was possible to obtain quite complete dishes of high nutritional value [13].
From the era of travelers and conquerors in the XV and XVI centuries, the mobilization of a great variety of foods began that ended up mixing and substantially modifying the way of eating of the entire population. The new diet integrated a great variety of native and foreign species [14]. That natural abundance invited to extend the culinary creativity to convert into a luxury what was at hand. Before the conquest, in the American continent, fats were not used in the preparation of food and they not were fried, so mixing the maize with lard turned out to be a radical change to the traditional diet [15]. On the other hand, beef, ram and pork were presented with abundance, so that their consumption became a daily habit in the food of the colonial era. With these proteins the stews became more complex, bittersweet, fatty and colorful [16,17].
With the development of the industrial revolution in the 19th century, the way of feeding underwent a new modification. On the one hand, the multiple wars left devastated nations, and the commercial blockades imposed by enemy countries caused a great famine due to a shortage of resources. These situations favored the search for low-cost foods that caused great satiety regardless of nutritional value [15]. In addition, the interconnection between countries and continents allowed the reception of a great influence of the culinary culture of other regions of the world. This communication made possible the creation of a new diet but still preserving the essence of the traditional dishes of each region. Foods such as milanesas, muffins, pizzas, cakes, hot cakes, chocolates, cheeses, sweet bread, medium-sized meats and pastries were introduced in places where they were not known, dishes that were characterized by their high carbohydrate and fat content [18].
The Food of today's World
Eating habits change as times modernize. Now, thanks to the industry, it is easy to find a wide variety of foods and very easily available, with the assumption of making life easier for the population [19]. The food of the modern world has changed completely. Food traditions have been abandoned to replace it with unhealthy customs. Currently, food is characterized by excessive consumption of sugar, saturated fat, salt and a significant decrease in fiber, natural water, fruits and vegetables [3].
Processed foods have led to the creation of diets with certain details, of which the so-called "westernized diet", this is characterized by an excessive consumption of poorly prepared red meats, sugary and carbonated beverages high in sodium and high-fructose corn syrup, saturated fats, refined sugar, and very low intake of fiber and natural water [15]. In addition, the preparation techniques that are used today such as deep frying breaded or weathered make the nutritional contribution of the food is lost due to the excess fat present in the food [20].
Industrialized food products are generally made with low quality ingredients, artificial sweeteners, and offer little nutritional value, which leads to an adaptation process which keeps people in constant consumption. Moreover, when the food consumed does not provide the necessary nutrients, it is difficult to reach satiety, resulting in overeating [21]. This process has had a significant impact on population health, contributing to the uncontrolled increase in overweight and obesity. This condition triggers a wide variety of metabolic disorders, including hyperglycemia, dyslipidemias. These alterations lead to the development of chronic non-communicable diseases such as diabetes mellitus, cardiovascular diseases, non-alcoholic fatty liver, and chronic kidney disease among others (Figure 1) [1].
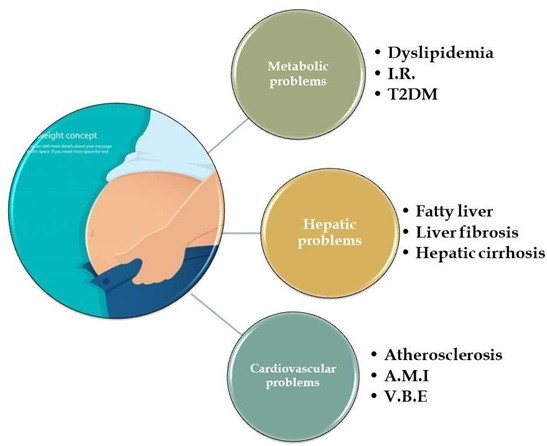
Figure 1: Main chronic non-communicable diseases associated with the development of obesity. I.R.: Insulin Resistance; T2DM: Type 2 Diabetes Mellitus; A.M.I.: Acute Myocardial Infarction; V.B.E.: Vascular Brain Event.
Food and Obesity
Epidemiology ofObesity
Obesity is a pathological condition characterized by excessive accumulation of adipose tissue in the body, particularly in the visceral region, which results in an increase in body weight [2]. Since 2003, obesity was stipulated as one of the greatest public health challenges worldwide, due to its accelerated increase and the problems it causes in health. Since then, obesity has been described as a global pandemic [22].
Worldwide, it is estimated that more than 1.9 billion adults have excess body weight, representing 76.3% of the total adult population [2]. Currently, Mexico and the United States of America have the first places in overweight and obesity worldwide, with a higher prevalence of 70%, being higher in women (75.6%) than in men (69.4%) [23]. It is estimated that obesity causes 3.4 million deaths per year in the world, and is responsible for 4% of lost years of life [24].
Pathophysiology of Obesity
Adipose tissue is well recognized as an active endocrine organ and the main warehouse and energy producer for the body [25]. This organ is formed by supportive reticular connective tissue called stroma, also to a wide variety of cell types such as fibroblasts, macrophages, mesenchymal cells and adipocytes, the latter being the main cell of adipose tissue. The main function of the adipocyte is to store excess energy in the form of triglycerides and then release them in situations of energy need [26]. Excess adiposity as an adverse consequence to health, is directly associated with the dysfunctional deposition of adipose tissue and the alteration in the secretion of factors related to inflammation [1]. These characteristics contribute to the development of several metabolic pathologies (Figure 2), circumstance that will be essential to determine the role of these alterations in the metabolic microenvironment, going from an anti-inflammatory to pro- inflammatory profile [27].
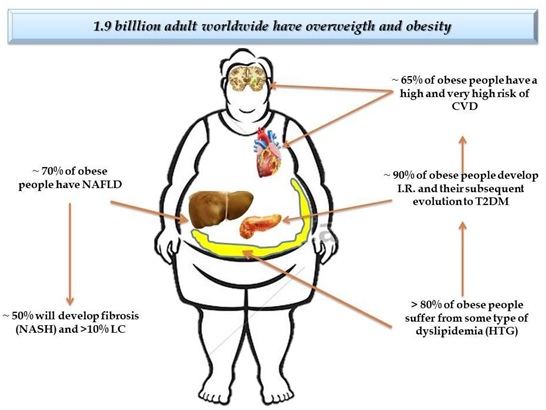
Figure 2: Excess adiposity as adverse consequence to health. NAFLD: Non Alcoholic Faty Liver Disease; NASH: Non Alcoholic Steatohepatitis; LC: Liver Cirrhosis; CVD: Cardiovascular Diseases; I.R.: Insulin Resistance; T2DM: Type 2 Diabetes Mellitus; HTG: Hypertriglyceridemia
Inside the genesis of obesity, the adipocyte can develop through two processes: hypertrophy (increase in size) and hyperplasia (increase in number) [28]. The adipocytes of the different fatty deposits of the body have a certain average size, a greater or lesser capacity for hypertrophy or hyperplasia, a differentiated secretory profile, and a greater or lesser relevance locally or systemically, depending on where they are [29]. This fact is very representative, since the accumulation of obesity in the abdominal region is related as the best predictor of cardiometabolic diseases associated with obesity [30].
Several studies have documented that a critical increase in adipocyte volume generates a hyperplasia process, which stimulates precursor cells by multiplying the cell number, and thus, the mass of adipose tissue [31]. Once the critical point is reached, the adipocyte apots a phenotype of hypertrophy, presents a dysfunction in its activity with decreased insulin sensitivity, cellular hypoxia, increased intracellular stress parameters, increased autophagy and apoptosis, as well as the increase in tissue inflammation [1,32].
Adipocyte hypertrophy, coupled with an inflammatory state, conditions its functioning, which alters the secretory hormonal profile by increasing leptin levels and decreasing adiponectin levels. The imbalance between these two hormones causes a lower sensitivity to insulin, leading to a decrease in mitochondrial function and increased endoplasmic reticulum stress [33]. This situation favors an increase in basal lipolysis, alteration of the cellular cytoskeleton and a lower de novo lipogenesis. This increase in baseline lipolysis is known as “hypotension of the overflow”, namely, the adipocyte saturates its ability to deposit triglycerides and these are directed to other tissues ectopically accumulating in abdominal organs, which generate lipotoxicity and insulin resistance (Figure 3) [34]. The increased flow of free fatty acids, together with pro-inflammatory factors, converts a situation of insulin resistance and local inflammation into a state of systemic insulin resistance and chronic low-grade inflammation [35].
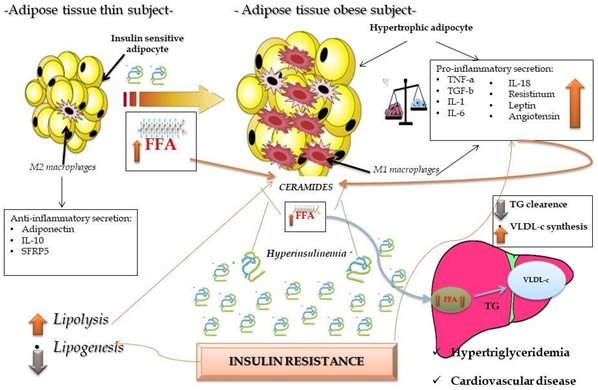
Figure 3: Pathophysiology of obesity. Phenotypic change of the adipocyte and its relation to the inflammatory state. FFA: Free Faty Acids; IL-10: Interleukine 10; SFRP5: Secreted frizzled-related protein 5; TNF-a: Tumor Necrosis Factor Alpha; TGF-b: Transforming Growth factor beta; IL-1: Interleukine 1; IL-6: Interleukine 6; IL-18: Interleukine 18; TG: Triglycerides; VLDL-c: Very Low Density Lipoprotein Cholesterol.
Due to its limited hyperplasic capacity, but high hypertrophic and inflammatory capacity, visceral adipose tissue becomes the first store of triglycerides due to the incompetence of subcutaneous adipose tissue to store excess energy (36). Its anatomical proximity to different organs, coupled with the high flow of pro- inflammatory factors, hypertrophied adipose tissue determines the systemic health of the individual [37]. Therefore, abdominal adiposity measures are directly and significantly related to mortality [38].
Eating Habits and the Development of Obesity
The development of obesity is multifactorial, where environmental factors play a determining role. Of these, the most relevant are an unhealthy diet with excessive calorie consumption, and poor or no physical activity [15]. The choice of food determines the diet, and therefore, the nutritional and health status of the population. Currently, obesity and an unhealthy diet are identified as one of the main 5 risk factors for general mortality worldwide [39]. There are social components that influence food preferences, some of them are customs, traditions, beliefs and culinary knowledge, as well as preferences determined by physiological and genetic aspects [15,40].
Eating habits such as poor fiber intake in the diet, excessive fat saturated consumption, fast food, carbonated drinks, alcohol, industrial pastries and the realization of less than five meals a day, are directly related to the development of obesity [41]. Processed foods high in saturated fats and refined sugars such as soft drinks, bottled juices and tea, hamburgers, hot dogs, pizza, cakes, instant soups and sugary cereals are some of the foods that favor excess body weight. This processed food is characterized by a deficiency in nutrients and that are currently part of the diet of the modern world [42].
Also to eating hypercaloric foods, there are other diet-related factors that seriously influence the development of obesity [43]. Meals outside the home have a remarkable role, since people often go to establishments that offer fast food. Besides, pre-cooked foods are increasingly used for ease and comfort. The pecking, which avoids main and complete meals in the course of the day and irregular meal times, make it common for people to skip meal times [3,44]. All these habits cause anxiety, and consequently make the diet excessively energetic, rich in simple sugars and saturated fats [45].
This type of “westernized diet” characterized by a high intake of simple sugars in the form of processed foods threatens the nutritional quality of diets [15]. The considerable amount of energy without nutrients provided by this type of food is evident, increasing the total caloric intake and reducing the intake of nutritionally healthy foods. Poor diet quality causes weight gain and, consequently, the development of obesity and an increase in the prevalence of chronic non- communicable diseases [1,3,42].
High-Fructose Corn Syrup as a Diet Element
Humans have a natural preference for sweet flavors. From birth, the child is fed breast milk which contains a great quantify of sugars, particularly lactose. Because of this, it is not surprising that as the individual grows, the preference for sweet flavors prevails [46]. Carbohydrates are fundamental in the diet of the human being. Its importance lies in the energy value, sweetening power and fiber content they have, so they constitute the major portion (50-60%) in a regular diet [47]. Despite the benefits offered by this macronutrient, the so-called simple carbohydrates have a direct implication with obesity when their consumption is excessive and out of control [48]. These sugars are characterized by rapid absorption and provide the body with only energy. In addition, they give a great sweet taste to food, and in particular in the industry they are added to improve the taste, texture and preservation of processed foods [49].
Fructose is the most used simple carbohydrate in processed food. Naturally, fructose is found in fruits and vegetables, which when ingested together with the fiber of these foods, their caloric intake and their level of intestinal absorption decreases considerably [50]. This property gives the sweet taste to fruits but without increasing the risk of developing pathologies related to metabolic alterations [51]. However, in the world of industry, fructose has been given a perverse use by indiscriminately adding it in the form of high-fructose corn syrup, due to its high sweet taste and low production cost [52]. The intake of high fructose corn syrup has increased considerably in recent years reaching 25% or more of the daily caloric intake (Table 1). Its excessive use in industry and high consumption of these products, have achieved a negative impact on the population health [53].
|
Comercial Product |
Portion |
Total Amount of Sugar in Grams |
Amount of Fructose in Grams |
|
Cookies |
4 pcs |
33.6 |
18.5 |
|
Cookies with oatmeal and apple |
8 pcs |
21.0 |
11.5 |
|
Chocolate cookies |
7 pcs |
42.7 |
23.5 |
|
Sweetmeats |
100 grs |
56.0 |
30.8 |
|
Chocolate |
2 pcs |
13.4 |
7.4 |
|
Soda |
330 ml |
36.3 |
19.9 |
|
Cola drink |
330 ml |
35.0 |
19.2 |
|
Bottled Te drink |
330 ml |
25.4 |
14.0 |
|
Energy drink |
473 ml |
52.0 |
28.6 |
|
Hamburger |
1 pc |
13.0 |
7.2 |
|
Individual pizza |
1 pc |
17.0 |
9.4 |
|
Natural yogurt |
280 ml |
36.0 |
19.8 |
|
Light yogurt |
280 ml |
29.7 |
16.3 |
|
Flan |
1 pc |
30.0 |
16.5 |
|
Drink with aloevera |
500 ml |
41.0 |
22.5 |
|
Chocolate donut |
1 pc |
17.0 |
9.3 |
|
Granola bar |
1 pc |
8.0 |
4.4 |
Table 1: Amount of total sugar and amount of fructose containing commercial products of frequent consumption. Pcs: Pieces; Pc: Piece, Grs: Grams; Ml: Milliliters.
One of the factors that have determined the constant consumption of foods containing high-fructose corn syrup is the high level of sweetness. This property leads to an increase in appetite, and therefore, to a higher intake of foods that contain this ingredient [54]. For this reason, high-fructose corn syrup has been directly associated with the development of obesity and its main comorbidities such as insulin resistance, diabetes mellitus, cardiovascular diseases and non- alcoholic fatty liver [53,55]. Unfortunately, high-fructose corn syrup is found in almost all industrialized foods and beverages with added sweeteners, which causes its consumption to be constant and frequent [56].
The World Health Organization recommends for adults and children, a consumption of simple sugars per day of 5% of the total caloric intake as maximum. That is, if an adult has a total requirement of 2,000 kilocalories per day, the intake of simple sugars would correspond to a maximum of 25 grams per day, this considering a contribution of 4 kcal/gr of carbohydrate [57]. Currently, the consumption of simple sugars exceeds 25% of the total caloric intake [53]. The combination of food intake with high-fructose corn syrup and a sedentary lifestyle, translates into a decrease in the metabolic demand of fat as a source of energy and a gain in body weight [58]. Consumption of this syrup causes a decrease in insulin secretion, which bring about an increase in blood glucose and a decrease in leptin [59]. Leptin's main function is to reduce food intake by inhibiting appetite [60]. By decreasing the concentration of leptin, the sensation of appetite is not reduced by having the need to continue eating. As a result, there is an increase of obesity [59,61].
It should be noted that foods that have the legend of "low fat" by reducing the content of this, contain the same amount of calories or even more than their original versions [52]. This is due to the fact that sugar content is commonly increased from high-fructose corn syrup to achieve an acceptable texture and flavor when removing fat, providing more calories. These foods become increasingly popular, and as a result they are much consumed, causing an increase in obesity rates [58].
Mesolimbic Dopaminergic System, Brain Reward and Food Addiction
Functioning of the Brain Reward System
The Brain Reward System (BRS) is responsible for mediating the feeling of pleasure in the body. This system is activated against actions that generate pleasure, such as eating delicious foods, playing sports, having sex or using stimulants such as drugs and alcohol. The BRS works in such a way that just thinking about the reward that is intended to get the feeling of pleasure is activated [62]. The motivation is closely related to the BRS, since it is in charge of directing the behavior towards the achievement of goals and obtaining rewards. In this way, the individual will perform the actions as they approach or move away to obtain a reward. The BRS also influences memory and learning. The individual remembers and repeats the actions that generate the sensation of pleasure and avoids those that produce an unpleasant sensation [63].
The BRS is anatomically constituted by dopaminergic neurons, also to serotonin, glutamate and dopamine, neurotransmitters that are grouped in the ventral tegmental area. These neurons project to the nucleus accumbens and to the amygdala, constituting the mesolimbic pathway. Moreover, the neurons of this system also have projection towards the prefrontal cortex, thereby forming the mesocortical pathway [64]. In the latter way, dopamine, neurotransmitter of greater relevance for the BRS, exerts its action on dopaminergic receptors type D1 (DRD1) with excitatory function, and type D2 (DRD2) with inhibitory function. The ventral tegmental area is activated when a rewarding action is performed, such as eating. Consequently, the release of dopamine in the nucleus accumbens increases, generating a feeling of pleasure and well-being [65].
Dopamine neurons activation generates several components of the reward, including the search for food and the reinforcement of teach. There are 5 types of dopamine receptors which have been identified and grouped into two families called D1 and D2. The D1 family receptors (Subtypes D1 and D5) are coupled to Gs proteins and stimulate cAMP synthesis as the main signal transduction mechanism. Subtypes belonging to the D2 family (D2, D3 and D4) inhibit cAMP synthesis [66]. Various alterations in this system have been related to diseases such as depression, bipolar disorder, and in particular, with addiction to psychoactive substances, gambling, sex and alcohol [6,67].
Affectation of the Brain Reward System in the Addictive Process
The addiction disorder is characterized by the lack of control over a certain behavior. At the beginning, this behavior is pleasant, but over time it takes over the individual's preferences until they dominate their behavior. Addictions seriously interfere with the person's daily life, significantly affecting their health [68]. When the addiction progresses, the behaviors become automatic, they are activated by impulses and emotions without cognitive control [69]. People normally perform a specific activity for pleasure or functionality. On the contrary, the addicted person does the activity to relieve their dysphoria or emotional discomfort [70].
The evidence accumulated in recent years allows us to affirm that addictive disorders of chronic course have their origin in the BRS [6,67]. While the initial use of a stimulant, such as a drug or a particular food, is voluntary, in the addictive state, the consumption of the stimulant is repeated more frequently increasing in each episode of its administration. This ultimately leads to modifications that last over time [71]. On the other hand, the induction of the addictive process does not depend exclusively on the stimulant itself, but also on factors of genetic vulnerability and external environmental variables [72].
Within the BRS there are necessary reinforcers and empty reinforcers that stimulate or inhibit the system. The necessary reinforcers are eating and sleeping. On the other hand, empty reinforcers include drugs, alcohol and money [73]. These empty reinforcers immensely activate the ventral tegmental area, which promotes a massive release of dopamine potentiating the pleasurable sensation [67]. It has been documented that during the withdrawal phase of these empty reinforcers, the reduction in the release of dopamine is manifested. This phenomenon has been linked to a dysphoric mood, which triggers withdrawal syndrome. This condition forces those empty reinforcers to be consumed again, increasing the tolerance thresholds, thereby establishing an addiction [74].
Food Addiction
The Dopaminergic Mesolimbic System (DMS) involving the Ventral Tegmental Area, Accumbens Nucleus, Amygdala and Prefrontal Cortex, plays an important role in food-addictive processes. It is described that in this brain region are governed the processes of gratification, pleasure, euphoria, joy, motor function, among others [75]. These pleasurable processes generated by food explain the behaviors that allow understanding survival in times of food shortages, as well as certain eating habits that lead to obesity. The activation of dopaminergic neurons in this cerebral region reinforces the pleasure generated by the stimulus of certain foods [5]. Thus, the sweet taste of some carbohydrates such as sugar, saccharin, fructose or high-fructose corn syrup have a particular stimulus in DMS that can lead to selecting certain foods repetitively until they develop an addiction to them, particularly those who are susceptible [76].
The secretion and capture of Dopamine at the synapse of the ATV and NA neuron stimulated by a sweet-tasting food has different pleasurable effect in individuals with different dopamine capture capacity at this synapse [69]. Studies with Positron Emission Tomography (PET) have shown that the pleasurable effect is longer in those with fewer D2 Dopamine receptors, which causes greater availability of dopamine in synapsis and perhaps recapture [66]. Variants have been described in the Dopamine Receptor Gene D2 (DRD2) associated with decreased number of dopamine D2 receptors in DMS, suggesting that carriers of this variant be more susceptible to develop addiction.
Recent studies show association of TaqIA DRD2/ANKK1 polymorphism with decreased D2 receptors and addiction to certain foods high in simple carbohydrates with "sweet" flavor and saturated fats, which could explain to some extent the development of obesity in those who prefer this type of food [5,76]. Food consumption, especially those rich in high-fructose corn syrup, and fat, activate the same dopamine circuits of the BRS involved in alcohol or drug addictions (Figure 4). Usually, feeding causes an increase in dopamine levels, which exerts an effect on the synapse of the nucleus accumbens [8]. The consumption of foods with very rewarding flavors, such as high-fructose corn syrup, leads to a gradual increase in dopamine until reaching a “tolerance” effect. This effect causes the dose of sugar to be gradually increased to achieve the desired satisfaction effect [77]. Chronic intake of these foods produces neuroadaptive changes that modify neuroplasticity by decreasing the function of the prefrontal cortex. The aforementioned compromises emotional and cognitive abilities of a higher order until they become automatism with a predominance of the negative effects of consumption [78].
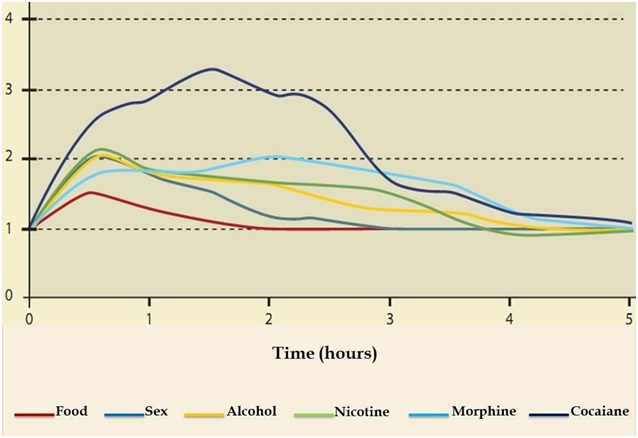
Figure 4: Dopamine neurotransmitter release induced by different reinforcers (necessary and empty). Recovered from: Mendez-Diaz M. (2017) Addiction neurobiology.
Within the food addictive process, the first neuroadaptive changes are manifested in the function of DRD1 and DRD2 [7]. Chronic consumption of foods high in sugar causes hyperstimulation of DRD1 that contributes to the degeneration of neuronal physiology. While DRD2, suffer a decrease in their expression. This contributes to the development of behavioral hyposensitivity, which causes overeating [79]. A complement to the addictive process orchestrated by dopamine has to do with the neurotransmitters serotonin and glutamate. Serotonin decreases control over the desire to eat foods rich in high-fructose corn syrup, and increases anxiety over its consumption. Meanwhile, glutamate enhances the neuronal pathways that link the memory of the consumption of these foods with the pleasure, which increases the desire to repeat the experience [80].
Clinical Management of the Obese Patient
Detachment to the Clinical-nutritional Treatment of the Obese Patient
The decrease in the prevalence of obesity is further complicated by the lack of adherence to the individual's clinical-nutritional treatment for the loss and control of body weight [6]. Commonly, the patient with obesity takes a passive attitude to his condition. This lack of interest reaches alarming figures, eight out of ten patients who start treatment leave before meeting the established goal. This situation contributes to maintaining and increasing the risks of chronic non- communicable diseases associated with obesity [81]. It has been documented that the lack of adherence to clinical-nutritional treatment is caused by different factors that include the economy, complexity of treatment, patient motivation, disease conditions and the type of participation of health professionals. Moreover, unrealistic expectations are involved, such as lifestyles incompatible with diet and, above all, compliance with body image that considerably reduce the success of short and long-term treatment [82].
Another aspect that influences adherence is the responsibilities and obligations of the patient, since they can cause attention to focus on issues outside their health such as work [83]. The lack of understanding that the patient has of the nature of the condition and frustration in the absence of clear and rapid results after starting a diet and exercise program, are other causes of detachment from dietary therapy [84]. Success in the treatment against obesity not only consists in a significant loss of body weight, but in the maintenance of long-term results. Regarding this last aspect, the situation is quite disappointing. Less than 30% of patients manage to keep the weight lost. In addition, 35% of treated patients recover the weight lost during the first year after treatment, and in a period of three to five years they usually reach a greater weight than the initial one [85].
Failures in the clinical-nutritional management of the obese patient are highly related to direct contact with foods rich in high-fructose corn syrup. The above, results in conditioned learning and the restoration of reward and motivation thresholds [80]. This results in an addiction with an inability to inhibit the urge to consume foods rich in sugars, leading to obesity [6].
Prospects of the Clinical-Nutritional Treatment of Obese Patients with Food Addiction
In the patient with food addiction, is convenient to gradually limit the consumption of foods rich in simple fats and sugars, since these reduce the availability of vitamins and minerals, favor the elevation of lipid levels, intensify anxiety and promote the development of cardiovascular diseases and other comorbidities [86]. Other stimulants are additives and artificial products that subtract nutrients and vitamins. It is important to avoid the consumption of monosodium glutamate, used to enhance flavors. This component has a strong irritative effect on the nervous system, producing, plus the addictive effect, headaches, paraesthesia and numbness [87].
Suitable foods in the diet of the obese patient are fruits and vegetables such as pineapple, banana, spinach, carrot, celery and broccoli [88]. These foods favor the absorption of tyrosine and tryptophan, precursors of dopamine and serotonin, neurotransmitters that regulate mood and anxiety [89]. In addition, lean meats, whole grains and legumes help to obtain energy in a natural and healthy way. In the integral management of food addiction it is important to add foods that contain calcium, a nutrient necessary to maintain an electrolyte balance, adequate muscle contraction and nerve transmission [87].
It is important to ensure a sufficiently balanced and complete diet in order to avoid nutritional deficiencies [90]. The lack of alpha-linoleic acid (omega 3) favors the appearance of panic attacks. Likewise, magnesium deficit causes agitation, anxiety, insomnia, confusion, depression and restlessness [91]. Vitamin B is important for the functioning of the nervous system and helps both relax and obtain energy daily [90]. Balanced nutrition is essential to maintain a general health, but also to be able to control food addictive disorders and regulate mood [15].
Cognitive behavioral therapy has treated overweight and obesity with promising results, decreasing excess body weight and modifying the way of eating [92]. However, the results are only maintained in the short term, possibly due to the presence of ambivalence in relation to the need to change [93]. On the other hand, the implementation of an anxiolytic drug treatment is essential; this to reduce relapses due to anxiety and food addiction [94]. Also prescribe medications to lose weight, if the patient requires it, as well as multivitamins in order to avoid their deficit [95].
CONCLUSIONS
The increase in obesity rates is closely related to food addiction. Codependency, easy access and the poor control that exists on the consumption of hypercaloric foods due to the high levels of pleasure that these cause to the individual, favor an uncontrollable increase in body weight gain, and therefore, an elevation in the prevalence of its main comorbidities. This addiction instrumented by the gratifying properties of the brain reward system, causes the increase in energy consumption without being able to control this action, causing the excessive increase in body weight. Therefore, food addiction and obesity should be understood as a result of habits that are strengthened by repeated behavior and that become increasingly difficult to control for the individual, despite its health consequences.
Current clinical-nutritional management is an inefficient treatment, since it does not have an impact on long-term weight control. Therefore, to combat obesity and its unhealthy consequences, it is necessary to implement a treatment with a multidisciplinary approach, with an approach from the perspective of food addiction, and from this, establish a specialized and individualized therapy.
ACKNOWLEDGMENTS
We thank the Secretary of Public Education of Mexico for the funding granted to conduct scientific research. Also thank the Nayarit Center of Innovation and Technology Transfer, Autonomous University of Nayarit (CENIT2-UAN) for providing the facilities for the use of information and communication technologies, as well as granting the spaces that house the Specialized Unit in Research, Development and Innovation in Genomic Medicine.
CONFLICTS OF INTEREST
The authors declare that they have no conflict of interest related to this study.
REFERENCES
- Jung UJ, Myung-Sook C. (2014). Obesity and Its Metabolic Complications: The Role of Adipokines and the Relationship between Obesity, Inflammation, Insulin Resistance, Dyslipidemia and Nonalcoholic Fatty Liver Disease. Int J Mol Sci. (15):6184-6223.
- World Health Organization. (2018). Obesity and overweight. Available from: URL: http://www.who.int/dietphysicalactivity/media/en/gsfs_obesity.pdf. [Accessed on 11/11/2019].
- Campos-Perez W, Gonzalez-Becerra K, Ramos-Lopez O, Silva-Gomez JA, Barron-Cabrera E, et al. (2016). Same Dietary but Different Physical Activity Pattern in Normal-weight and Overweight Mexican Subjects. Food Nutr Res. (4):729-735.
- Lee NM, Carter A, Owen N, Hall WD. (2012). The neurobiology of overeating. Treating overweight individuals should make use of neuroscience research, but not at the expense of population approaches to diet and lifestyle. EMBO Rep. (9):785–790.
- Ramos-Lopez O, Mejia-Godoy R, Frias-Delgadillo KJ, Torres-Valadez R, Flores-Garcia A, et al. (2019). Interactions between DRD2/ANKK1 TaqIA Polymorphism and Dietary Factors Influence Plasma Triglyceride Concentrations in Diabetic Patients from Western Mexico: A Cross-sectional Study. Nutrients. (11):E2863.
- Panduro A, Rivera-Iñiguez I, Sepulveda-Villegas M, Roman S. (2017). Genes, emotions and gut microbiota: The next frontier for the gastroenterologist. World J Gastroenterol. (23):3030-3042.
- Blum K, Thanos PK, Gold MS. (2014). Dopamine and glucose, obesity, and reward deficiency syndrome. Frontiers in Psychology. (5):919.
- Benton D, Young H. (2016). A meta-analysis of the relationship between brain dopamine receptors and obesity: a matter of changes in behavior rather than food addiction? Int J Obes. (40):S12–S21.
- Martínez M, García-Cedillo I, Estrada-Aranda B. (2016). Adherence to nutritional therapy: Intervention based on motivational interviewing and brief solution-focused therapy. Mexican J Eating Disord. (7):32-39.
- Reich D, Patterson N, Campbell D, Tandon A, Mazieres S, et al. (2012). Reconstructing Native American population history. Nature. (488):370-374.
- Garcia-Moll R. (2007). Early and middle preclassic (2500-400 BC): The first agricultural societies. Arqueología Mexicana. (15):34-43.
- Carrillo-Trueba C. (2009). The origin of maize, nature and culture in Mesoamerica. Ciencias. (92):4-13.
- Servín Rodas M.C. (2013). Nutrición básica y aplicada [Spanish], [2]. Universidad Nacional Autónoma de México, Federal District, México, 23-31.
- Sanchez-Albornoz N. (1974). The population of Latin America: A history. University of California Press, Berkeley, California, USA, 1-299.
- Roman S, Ojeda-Granados C, Ramos-Lopez O, Panduro A. (2015). Genome- based nutrition: An intervention strategy for the prevention and treatment of obesity and nonalcoholic steatohepatitis. World J Gastroenterol. (12):3449- 3461.
- Gomez-Delgado Y, Velazquez-Rodriguez E.B. (2019). Health and food culture in Mexico. Rev Digital Univeritaria. (20):1-11.
- Quiroz E. (2014). Eating in New Spain, privileges and regrets of society in the XVIII century. Rev Hist Mem. (8):19-58.
- Martínez-Cortés G, Salazar-Flores J, Fernández-Rodríguez LG, Rubi- Castellanos R, Rodríguez-Loya C, et al. (2012). Admixture and population structure in Mexican-Mestizos based on paternal lineages. J Hum Genet. (57):568-574.
- Lichtenstein AH, Kennedy E, Barrier P, Danford D, Ernst ND, et al. (1998). Dietary fat consumption and health. Nutr Rev. (56):S19- S28.
- Flores M, Macias N, Rivera M, Lozada A, Barquera S, Rivera-Dommarco J, et al. (2010) Dietary patterns in Mexican adults are associated with risk of being overweight or obese. J Nutr. (140):1869–1873.
- Kanoski Scott E, Davidson Terry L. (2011). Western Diet Consumption and Cognitive Impairment: Links to Hippocampal Dysfunction and Obesity. Physiol Behav. (103):59-68.
- Malik V.S, Willett W.C, Hu F.B. (2013). Global obesity: trends, risk factors and policy implications. Nat Rev Endocrinol. (9):13-27.
- Organization for Economic Cooperation and Development (OECD). (2017). Health at a Glance 2017: OECD Indicators. OECD. Available from: URL: https://www.oecd.org/mexico/Health-at-a-Glance-2017-Key-Findings.pdf. [Accessed on: 25/11/2019].
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, et al. (2014). Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet. (14):1-16.
- Spalding KL, Arner E, Westermark PO, Bernard S, Buchholz BA, et al. (2008). Dynamics of fat cell turnover in humans. Nature. (453):783–787.
- Hurt RT, Frazier TH, McClave SA, Kaplan LM. (2011). Obesity epidemic: overview, pathophysiology, and the intensive care unit conundrum. J Parenter Enteral Nutr. (35):S4-S13.
- Lumeng CN, Saltiel AR. (2011). Inflamatory links between obesity and metabolic disease. J Clin Invest. (6):2111-2117.
- Gonzalez-Jimenez E. (2013). Obesity: etiologic and pathophysiological analysis. Endocrinol Nutr. (1):17-24.
- Tchoukalova YD, Votruba SB, Tchkonia T, Giorgadze N, Kirkland JL, et al. (2010). Regional differences in cellular mechanisms of adipose tissue gain with overfeeding. Proc Natl Acad Sci. (107):18226–18231.
- Manzur F, Alvear C, Alayón AN. (2010). Adipocytes, visceral obesity, inflammation and cardiovascular disease. Rev Colomb Cardiol. (17):207-213.
- Rosen ED, Spiegelman BM. (2014). What we talk about when we talk about fat. Cell. (156):20-44.
- Bays HE, Toth PP, Kris-Etherton PM, Abate N, Aronne LJ, et al. (2013). Obesity, adiposity, and dyslipidemia: A consensus statement from the National Lipid Association. J Clinc Lipid. (7):304-383.
- Lehr S, Hartwig S, Sell H. (2012). Adipokines: a treasure trove for the discovery of biomarkers for metabolic disorders. Proteomics Clin Appl. (6):91-101.
- Grundy SM. (2016). Overnutrition, ectopic lipid and the metabolic syndrome. J Investig Med. (64):1082-1086.
- Schipper HS, Prakken B, Kalkhoven E, Boes M. (2012). Adipose tissue- resident immune cells: Key players in immunometabolism. Trends Endocrinol Metab. (23):407–415.
- Laforest S, Labrecque J, Michaud A, Cianflone K, Tchernof A. (2015). Adipocyte size as a determinant of metabolic disease and adipose tissue dysfunction. Crit Rev Clin Lab Sci. (6):301-313.
- Moreno-Indias I, Tinahones FJ. (2015). Impaired adipose tissue expandability and lipogenic capacities as ones of the main causes of metabolic disorders. J Diabetes Res. (1):1-12.
- Carmienke S, Freitag MH, Pischon T, Schlattmann P, Fankhaenel T, et al. (2013). General and abdominal obesity parameters and their combination in relation to mortality: a systematic review and meta- regression analysis. Eur J Clin Nutr. (6):573–585.
- The Burden of Disease Project [WWW document]. (2010). Available from: URL: http://www.healthmetricsandevaluation.org/gbd/visualizations/gb d-arrow-diagram. [Accessed on 05/09/2018].
- Gutiérrez-Valverde JM, Guevara-Valtier MC, Enríquez-Reyna MC, Ángeles Paz-Morales MA, Hernández-del Ángel MA, et al. (2017). Study of families: Environmental and Cultural Factors associated with Overweight and Obesity. Enferm glob. (16):11-19.
- Jáuregui-Lobera I, Bolaños Ríos P. (2011). What motivates the consumer's food choice?. Nutr Hosp. (6):1313-1321
- Monteiro CA, Moubarac JC, Cannon G, Ng SW, Popkin B. (2013). Ultra- processed products are becoming dominant in the global food system. Obes Rev. (14):21-28.
- Ramos-López O, Román S, Ojeda-Granados C, Sepúlveda-Villegas M, Martínez-López E, et al. (2013). Patrón de ingesta alimentaria y actividad física en pacientes hepatópatas en el Occidente de México. Rev. Endocrinol Nutr. (21):7–15.
- Carrera PM, Gao X, Tucker KL. (2007). A study of dietary patterns in the Mexican-American population and their association with obesity. J Am Diet Assoc. (107):1735-1742.
- Flores M, Macias N, Rivera M. (2010). Dietary patterns in Mexican adults are associated with risk of being overweight or obese. J Nutr. (140):1869-1873.
- Drewnowski A, Mennella JA, Johnson SL, Bellisle F. (2012). Sweetness and food preference. J Nutr. (142):1142S–1148S.
- Mann J, Cummings JH, Englyst HN, Key T, Liu S, et al. (2007). FAO/WHO Scientific Update on carbohydrates in human nutrition: conclusions. European J Clin Nutr. (61):S132–S137.
- Ramos-Lopez O, Panduro A, Martinez-Lopez E, Roman S. (2016). Sweet Taste Receptor TAS1R2 Polymorphism (Val191Val) Is Associated with a Higher Carbohydrate Intake and Hypertriglyceridemia among the Population of West Mexico. Nutrients. (8):1-12.
- Cabezas-Zabala CC, Hernandez-Torres BC, Vargas-Zarate M. (2016). Sugars added in food: health effects and global regulation. Rev Fac Med. (64):319-329.
- Johnson RJ, Lanaspa MA, Roncal-Jimenez C, Sanchez-Lozada LG. (2012). Effects of excessive fructose intake on health. Ann Intern Med. (156):905–906.
- Goran MI, Tappy L, Le KA. (2015). Dietary Sugars and Health. [1], CRC Press, Taylor & Francis Group, Boca Raton, Florida, USA, 99.
- Rippe JM, Angelopoulos TJ. (2013). Sucrose, high-fructose corn syrup, and fructose, their metabolism and potential health effects: what do we really know?. Adv Nutr. (4):236–245.
- Malik VS, Hu FB. (2015). Fructose and Cardiometabolic Health: What the Evidence From Sugar-Sweetened Beverages Tells Us. J Am Coll Cardiol. (66):1615–1624.
- White JS. (2013). Challenging the fructose hypothesis: new perspectives on fructose consumption and metabolism. Adv Nutr. (4):246-56.
- Choo VL, Viguiliouk E, Blanco-Mejia S, Cozma AI, Khan TA, et al. (2018). Food sources of fructose-containing sugars and glycaemic control: systematic review and meta-analysis of controlled intervention studies. BMJ. (363):k4644.
- Riveros MJ, Parada A, Pettinelli P. (2014). Fructose consumption and its health implications: fructose malabsorption and nonalcoholic fatty liver disease. Nutr Hosp. (29):491-499.
- World Health Organization. (2015). Intake of sugars for adults and children. Available
- Lisbona-Catalán A, Palma-Milla S, Parra-Ramírez P, Gómez-Candela C. (2013). Obesity and sugar: allies or enemies Nutr Hosp. (28):81-87.
- Shapiro A, Mu W, Roncal C, Cheng KY, Johnson RJ, et al. (2008). Fructose-induced leptin resistance exacerbates weight gain in response to subsequent high-fat feeding. Am J Physiol Regulo Integr Comp Physiol. (295):1370–1375.
- Friedman JM, Halaas JL. (1998). Leptin and the regulation of body weight in mammals. Nature. (395):763–770.
- Tillman EJ, Morgan DA, Rahmouni K, Swoap SJ. (2014). Three months of high-fructose feeding fails to induce excessive weight gain or leptin resistance in mice. PloS One. (9):e107206.
- van der Laan LN, de Ridder DT, Viergever MA, Smeets PA. (2014). Activation in inhibitory brain regions during food choice correlates with temptation strength and self-regulatory success in weight-concerned women. Front Neurosci. (8):308.
- Schoenbaum G, Roesch M. (2005). Orbitofrontal cortex, associative learning, and expectancies. Neuron. (47):633-636.
- Russo SJ, Nestler EJ. (2013). The brain reward circuitry in mood disorders. Nat Rev Neurosci. (14):609-625.
- Oganesyan GA, Romanova IV, Aristakesyan EA, Kuzik VV, Makina DM, et al. (2009). The dopaminergic system of the telencephalon- diencephalic areas of the vertebrate brain in the organization of the sleep- waking cycle. Neurosci Behav Physiol. (39):805-817.
- Hyman SE, Malenka RC, Nestler EJ. (2006). Neural mechanisms of addiction: the role of reward-related learning and memory. Annu Rev Neurosci. (29):565-598.
- Gardner EL. (2011). Addiction and brain reward and antireward pathways. Adv Psychosom Med. (30):22-60.
- Grant JE, Potenza MN, Weinstein A, Gorelick DA. (2010). Introduction to behavioral addictions. Am J Drug Alcohol Abuse. (36):233–241.
- Konkolÿ-Thege B, Woodin EM, Hodgins DC, Williams RJ. (2015). Natural course of behavioral addictions: a 5-year longitudinal study. BMC psychiatry. (15):4.
- Volkow ND, Wang GJ, Fowler JS, Tomasi D. (2012). Addiction circuitry in the human brain. Annu Rev Pharmacol Toxicol. (52):321–336.
- Olsen CM. (2012). Natural rewards, neuroplasticity, and non-drug addictions. Neuropharmacology. (61):1109–1122.
- MacKillop J. (2013). Integrating behavioral economics and behavioral genetics: delayed reward discounting as an endophenotype for addictive disorders. J Exp Anal Behav. (99):14–31.
- Seo H, Lee D. (2009). Behavioral and neural changes after gains and losses of conditioned reinforcers. J Neurosci. (29):3627–3641.
- Lek FY, Ong HH, Say YH. (2018). Association of dopamine receptor D2 gene (DRD2) TaqI polymorphisms with eating behaviors and obesity among Chinese and Indian Malaysian university students. Asia Pac J Clin Nutr. (2):707–717.
- Sun X, Luquet S, Small DM. (2017). DRD2: Bridging the Genome and Ingestive Behavior. Trends Cong Sci. (5):372-384.
- Rivera-Iñiguez I, Panduro A, Ramos-Lopez O, Villaseñor Bayardo SJ, Roman S. (2019). DRD2/ANKK1 Taq1 polymorphism associates with overconsumption of unhealthy foods and biochemical abnormalities in a Mexican population. Eat Weight Disord. (5):835-844.
- Ifland JR, Preuss HG, Marcus MT, Rourke KM, Taylor WC, et al. (2009). Refined food addiction: A classic substance use disorder. Med Hypotheses. (72):518–526.
- Burrows T, Skinner J, McKenna R, Rollo M. (2017). Food Addiction, Binge Eating Disorder, and Obesity: Is There a Relationship? Behav Sci. (7):54.
- Davis C, Loxton NJ, Levitan RD, Kaplan AS, Carter JC, et al. (2013). “Food addiction” and its association with a dopaminergic multilocus genetic profile. Physiol Behav. (118):63–69.
- Gordon EL, Ariel-Donges AH, Bauman V, Merlo LJ. (2018). What Is the Evidence for "Food Addiction?" A Systematic Review. Nutrients. (10):477.
- Martínez M, García-Cedillo I, Estrada-Aranda B. (2016). Adherence to nutritional therapy: Intervention based on motivational interviewing and brief solution-focused therapy. Mexican J Eating Disord. (7): 32-39.
- Barnes R, Ivezaj V. (2015). A systematic review of motivational interviewing for weight loss among adults in primary care. Obes Rev. (16):304–318.
- Hill B, Skouteris H, Fuller-Tyszkiewicz M. (2013). Interventions designed to limit gestational weight gain: a systematic review of theory and meta- analysis of intervention components. Obes Rev. (14):435–50.
- Barrios-Vicedo R, Navarrete-Muñoz EM, García de la Hera M, González- Palacios S, Valera-Gran D, et al. (2014). A lower adherence to Mediterranean diet is associated with a poorer self-rated health in universirty population. Nutr Hosp. (31):785–792.
- Sámano-Orozco LF. (2011). Abandoning diet treatment of patients with diagnosed obesity in the nutritionist private office. Nutr Clin Diet Hosp. (31):15-19.
- Adams RC, Lawrence NS, Verbruggen F, Chambers CD. (2017). Training response inhibition to reduce food consumption: Mechanisms, stimulus specificity and appropriate training protocols. Appetite. (109):11–23.
- Adams RC, Sedgmond J, Maizey L, Chambers CD, Lawrence NS. (2019). Food Addiction: Implications for the Diagnosis and Treatment of Overeating. Nutrients. (11):2086.
- Kakoschke NL, Kemps E, Tiggemann M. (2017). The effect of combined avoidance and control training on implicit food evaluation and choice. J Behav Ther Exp Psychiatr. (55):99–105.
- Hardman CA, Herbert VM, Brunstrom JM, Munafò MR, Rogers PJ, et al. (2012). Dopamine and food reward: Effects of acute tyrosine/phenylalanine depletion on appetite. Physiol Behav. (105):1202– 1207.
- Esper DH. (2015). Utilization of nutrition-focused physical assessment in identifying micronutrient deficiencies. Nutr Clin Pract. (30):194–202.
- Reber E, Gomes F, Vasiloglou MF, Schuetz P, Stanga Z. (2019). Nutritional Risk Screening and Assessment. J Clin Med. (8):1065.
- Castelnuovo G, Pietrabissa G, Manzoni GM, Cattivelli R, Rossi A, et al. (2017). Cognitive behavioral therapy to aid weight loss in obese patients: current perspectives. Psychol Res Behav Manag. (10):165–173.
- Knowles L, Anokhina A, Serpell L. (2013). Motivational interventions in the eating disorders: What is the evidence? Int J Eat Disord. (46):97–107.
- Rodgers RJ, Tschöp MH, Wilding JP. (2012). Anti-obesity drugs: past, present and future. Dis Model Mech. (5):621–626.
- Srivastava G, Fox CK, Kelly AS, Jastreboff AM, Browne AF, et al. (2019). Clinical Considerations Regarding the Use of Obesity Pharmacotherapy in Adolescents with Obesity. Obesity (Silver Spring). (27):190–204.
Copyright: Torres-Valadez R, et al. ©2020. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Torres-Valadez R (2020). Obesity and Food Addiction: Consumption of High-Fructose Corn Syrup and the Effectiveness of Clinical-Nutritional Management. Clin Res 1(1): 01.