2023: Volume 4, Issue 4
Past Issues
 Abstract
Abstract  PDF
PDFEffects of Led Light Screens on School Children Eyes
Cristina Bonnin-Arias, Vanesa Blázquez Sánchez*, Xavier Rodríguez Alonso, Sara Gutiérrez Jorrin, Celia Sánchez Ramos
Grupo de visión y oftalmología de la Facultad de Óptica-Optometría de la Universidad Complutense de Madrid, Spain
*Corresponding Author: Grupo de visión y oftalmología de la Facultad de Óptica-Optometría de la Universidad Complutense de Madrid, Spain; Email: [email protected]
Received Date: August 5, 2023
Publication Date: November 9, 2023
Citation: Bonnin-Arias C, et al. (2023). Effects of Led Light Screens on School Children Eyes. Clin Res. 4(4):20.
Copyright: Bonnin-Arias C, et al. © (2023).
ABSTRACT
Background: The increasing use of digital devices involves a potential risk for public health. Screens are generally made with LED lights, with a peak of emission in the area of visible spectrum corresponding to blue light. Given the high amount of blue light energy, several studies suggest a subsequent phototoxic damage to the retina. Blue light radiation may have greater impact on children particularly given that retina is not entirely developed at this age, larger pupillary diameters and frequent shorter viewing distances when compared to adults. Methods: The amount of blue light potentially penetrating the eye of adults and children was assessed. Light amounts reaching the eye were theoretically calculated according to measured pupillary diameters and reading distances. Results: The amount of visible radiation reaching the pupil is theoretically 1.4 times higher when using a smartphone than when using a PC. Light amount reaching the eye depends on reading distance. The shorter reading distance, the higher light amount reaches the eye. Children are likely exposed to a 40% higher light dose than adults because of their body-anatomic features. Conclusions: Exposure to LED screen devices should be particularly considered among children. Long-term effects of blue light exposure should me more carefully investigated.
BACKGROUND
The use of computers and electronic devices has not stopped increasing over the last decades. Electronic devices are essential in modern academic, professional and social life. In terms of public health, the use of digital devices is no longer limited to adults but also to young people and children. Technological devices have widely diversified from desktop computers (PC) to laptops, tablets, smartphones, videogames, etc. Whether at work or home, electronic devices and digital screens are everywhere [1,2].
Portable devices such as smartphones or tablets usually display little reading texts (according to screen dimensions), generally forcing the observer to reduce the viewing distance or to use magnifying tools, if available. This is especially common among children because of their anatomic characteristics (short arm length) and when using touch devices. A short reading distance requires a higher visual effort to focus.
As a result of a long-term reading effort, a variety of symptoms may arise. These symptoms have been termed as “Computer Vision Syndrome” (CVS) [1].

Figure 1: Viewing distance of an 18-month-old child. The touch screen forces the child to reduce the viewing distance.
Current displays use light-emitting diodes (LEDs), with a very specific emission spectrum and energy characteristics. Since there are no LEDs emitting white light as such, they are initially made by using blue light, with an emission peak around 450-470 nm3, the highest energetic area within the visible spectrum. To obtain a subsequent white light perception, blue LEDs are combined with a yellow phosphor coating, with an emission wave length peak around 580 nm4. As a result of this, LED emission spectrum is considerably different to other traditional lighting systems such as fluorescent or incandescent white light sources (despite their similar appearance).
The visual effects of LED light exposure are being thoroughly investigated. Several epidemiological studies suggest that both ultraviolet radiation and visible light can damage the retina through photochemical [5], thermal and mechanical mechanisms [6]. Furthermore, it has been shown that the retina is not equally sensitive to the entire visible spectrum. Retina is much more sensitive to short wavelengths such as blue light [7].
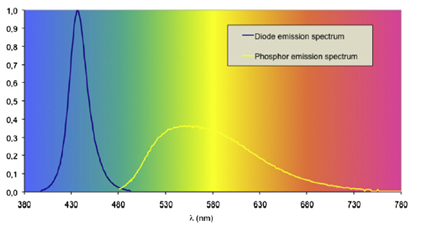
Figure 2: White light spectral representation as a combination of a blue light diode and a yellow phosphor coating. Taken from Behar-Cohen, 2011.
Potential injuries from light exposure depend on several factors. First, the eyes have to be exposed to a certain type of light (a potentially harmful wavelength). Thus, any possibility of retinal injury depends on the screen’s wavelength emission. Eye development is a second factor to take into account. Retinal maturity is reached at 45 months of age []8 (cone density is 80% less at birth than in adulthoold). For this reason, children are more sensitive to LED light phototoxicity than fully developed adult structures [9]. Then, the pupillary diameter must be considered. Pupillary diameter decreases with age linearly. Adult pupillary diameter reductions are more evident on scotopic conditions. Because of that, children receive greater amounts of retinal illumination [10]. Finally, the amplitude of accommodation has to be considered. Higher accommodation abilities allow children to read at closer distances [11,12].
Taking all these factors into account, this study aims to evaluate the amount of blue light (450 nm wavelength) emitted by the LED screens reaching the eye pupil and to compare these measurements with those obtained when reading on paper.
MATERIALS AND METHODS
MATERIALS
Measurements were taken with the Ocean Optics USB2000 spectrophotometer installed on a millimeter optical bench. The optical bench included two pieces to place the screen (mobile piece to modify position) and the light detector. The software used for the visualization of the emission curves was Spectrasuite.

Figure 3: Spectrophotometer Ocean Optics USB 2000 installed on the optical bench was used to measure the screen’s light emission.
A random selection of traded screen devices was conducted. The selected smartphone was the Huawei p8 lite 2017 (Huawei, China), FHD screen, 5.2 inches and resolution of 1920x1080 pixels; the selected tablet was the Vexia Tab 9i (Vexia, Spain), IPS LED display, 9-inch resolution 1920x1200 pixels; and the selected computer was the ASUS F540SA-XX445T, LCD screen LED, 15.6 inches and resolution of 1366x768 pixels .
METHODS
The effects of radiation from LED screens on the eyes depend on the spectral composition of the light, the usage time and the working distance. The amount of radiation entering the eye is proportional to the pupil diameter and inversely proportional to the viewing distance.
Measurements were taken in the laboratory of the Group of Neuro-Computation and Neuro-Robotics. All devices were switched on 10 minutes before starting to take any measurements. To standardize light emission levels, all devices were programmed to emit a completely white image, with equal brightness values. Peak emission wavelengths (between 446 nm and 450 nm) from all screen devices were analyzed. Measurements were made in triplicate at three different points on the screens for a total of 11 distances between 1 and 50 cm in steps of 5 cm.
To calculate the illumination reaching the eye, the value of the quantas of light (450nm) measured at each of the studied distances and the pupil diameter, by which this value is multiplied, were taken into account. The pupillary diameters used for all calculations were 2.5 mm, 4 mm and 5.5 mm , considering that the mean pupillary diameter can vary between 2 mm and 8 mm depending on the level of illumination and age, obtaining the highest visual acuities with diameters between 2 and 4 mm [13].
Finally, the same measurements were taken to analyze the light reflected by the paper at the usual reading distances of children (20-30 cm) and adults (30-40 cm). Paper and screen reflected light emissions were compared.
RESULTS
Once measurements were made, the amount of light reaching the eye was calculated. The graphs obtained for pupillary diameters of 4 ± 1.5 mm are shown below.
The estimated working distances for each device were as follows:
• Smartphones: 25-35 cm
• Tablets: 30-40 cm
• Computers: 45-50 cm
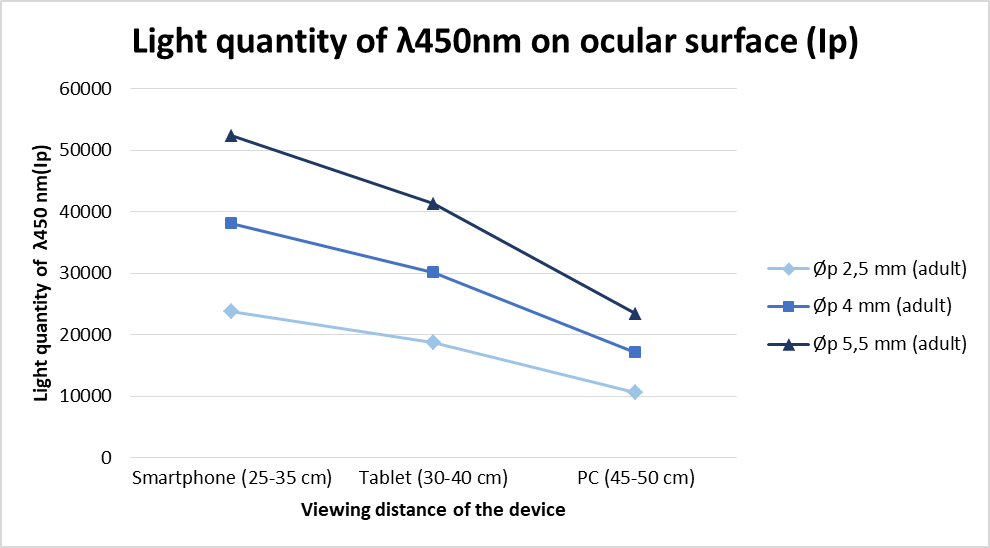
Figure 4: Light quantity of λ 450 nm penetrating the eye as a function of the pupillary aperture (mm) and the viewing distance (cm).
Figure 4 represents how the larger pupillary diameter is, the more light penetrates the eye. Light dose increases when the device approaches the eye. For the laptop working distance (45-50 cm), the amounts of light reaching the pupil were 23431.1; 17040.8 and 10650.5 for pupil diameters of 5.5 mm, 4 mm and 2.5 mm, respectively. For shorter working distances such as when using a smartphone (25-35 cm), the amount of light entering the eye was 52461.3, 38153.7 and 23846.1 when pupillary diameters were 5.5 mm, 4 mm and 2.5 mm, respectively. The amount of light that reaches the eye pupil when an adult uses a smartphone is theoretically 1.4 times greater than that when using a computer.
The same calculations were made for a child reading distance. Therefore, reading distances were reduced by approximately 10 cm.

Figure 5: School-age children using tablets for study or leisure activities at distances less than 15-20 cm.
The following chart shows the amount of light reaching the eye as a function of the pupil diameter and the reading distance. The results show values of 72338.0; 52609.5 and 32880.9 for the use of smartphones (15-20 cm), 43826.0; 31873.5 and 19920.9 quantas• mm for the use of tablets (20-30 cm) and 23686.0; 17226.2 and 10766.4 when using PC-LED displays (30-40 cm), considering pupils of 5.5 mm, 4 mm and 2.5 mm, respectively.
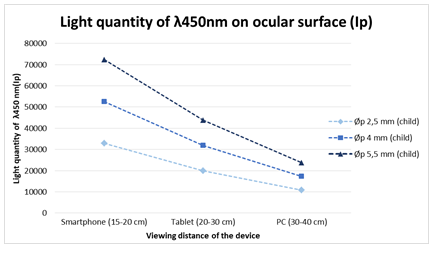
Figure 6: Light quantity of λ 450 nm penetrating the eye as a function of the pupillary aperture and the viewing distance of LED screen devices by children.
The graph below shows, for each device, that the larger the pupillary diameter and the shorter reading distance, the greater the amount of light enters the eye. This study has not included the pupillary diameter reduction due to screen illumination and the accommodation reflex. Children receive 40% more light than adults when using smartphones due to reduced reading distance.
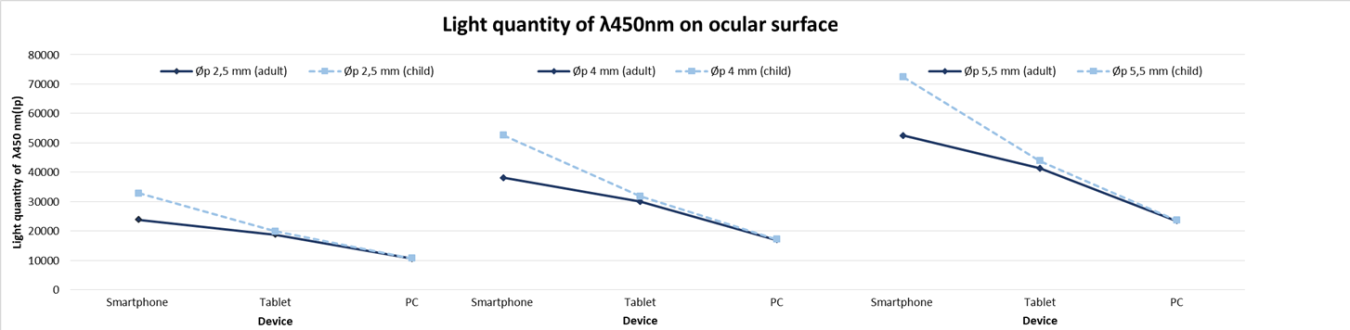
Figure 7: Children vs adults. A light entering the eye comparison when PC’s, tablets and smartphones are used.
The following data tables show pupil diameters, viewing distances and the light amounts entering the eyes. The smallest pupillary diameters (2.5 mm) were selected for the smartphones and tablets usage because of the increased pupillary stimulation when light devices are placed near the eyes.
Table: Light quantity of λ 450 nm penetrating the eye according to the pupillary diameters of 2.5 mm and the most frequent distances during the use of smartphones and tablets with LED screens.
|
Smartphone (children) |
Smartphone (adult) |
Tablet (children) |
Tablet (adult) |
Computer (children) |
Computer (adult) |
|
|
øp (mm) ) |
2,5 |
2,5 |
2,5 |
2,5 |
5,5 |
4 |
|
Distancias (cm) |
15-20 |
25-35 |
20-30 |
30-40 |
30-40 |
45-50 |
|
Ip (cuantas·mm) |
32880.9 |
23846.1 |
19920.9 |
18771.9 |
23686.0 |
17040.8 |
Light quantity of λ 450 nm penetrating the eye according to the pupillary diameters of 4 mm and 5.5 mm and the most frequent distances during use of PC.
On the other hand, the amount of light reflected off the paper was measured under photopic illumination conditions, similar to those of a conventional classroom. Paper light reflection was compared to that obtained when reading on a tablet at the same distance (between 20 and 30 cm in the case of children and between 30 and 40 cm in that of adults). It has been estimated that children receive approximately 7.5 times more blue light (450 nm) when reading on a tablet than when reading on paper.
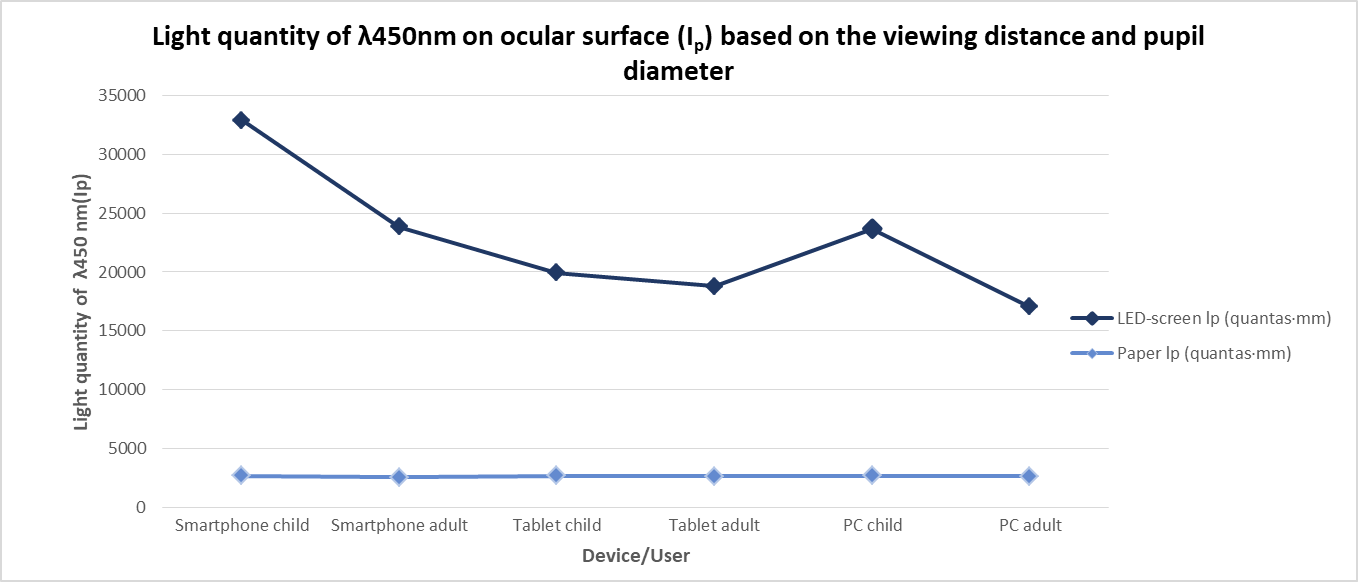
Figure 8: Light amount (λ 450 nm) that penetrates the eye of children and adults depending on the most frequent parameters of pupillary aperture and the distance of use of the LED devices against the light reflected by the paper for the reading distances of children and adults. The reading distances are always between 20 and 30 cm for children and between 30 and 40 cm for adults.
DISCUSSION
Classical and current studies in the United States show that only 18% of households had computers in 1997. In 2009, this percentage increased to 68.7% and, in 2013, 83.8% [14]. In Europe and the rest of the world, similar data has been reported. Recent research among more than 2.000 children aged 8-18 years reported a daily LED screen usage of 7.5 hours, for both academic and leisure activities (4.5 hours watching television, 1.5 hours using laptops, and more than one hour playing video games) [1,15].
This study evaluates theoretically the amount of light from LED screen devices potentially penetrating the eye and the role of the pupil diameter and the viewing distance.
First, the pupillary diameter decreases linearly with age, with a decrease of 0.015 to 0.043 mm per year under low illumination conditions [16]. These differences are less evident under photopic conditions. Since children have a larger pupillary diameter, they could potentially be exposed to a higher dose of blue light.
Regarding the reading distance, this study has established the same measures provided on other studies [17-19]. It has been described before how a reduced viewing distance is normally related to a shorter arm length and higher accommodation ability [11]. These anatomical and functional conditions predispose the retina to increased exposure light
Our results confirm that blue light potentially reaching the retina depends on the reading distance and the pupillary diameter. Children may be especially susceptible because of their larger pupillary diameter, the shorter reading distance and the lack of lens deterioration (yellowing) acting as a protective filter.
Furthermore, there is a chronic cumulative effect on the ocular structures. A harmful effect of blue light may accumulate over time, with more dangerous consequences on developing structures. The use of these devices may cause an irreversible damage to the retina. In recent years, numerous animal experiments have shown a photoreceptor layer thickness decrease after a long-term LED light exposure [20,21]. Activation of cell death by necrosis and apoptosis at a molecular level have been also reported [22-24].
There is a global growing trend towards the general use of electronic devices in schools and education. Learning based on these devices is a sign of technological development. Determining the best strategies to successfully implement digital devices in order to improve learning is a booming research topic [25]. Symptoms such as those related to accommodative, vergence dysfunction and dry eye are particularly worth noting problems [26].
In short, children exposure to harmful radiation has increased in recent years due to the use of digital devices. Cumulative photoxic retinal damage and blue LED-light exposure must be more investigated.
CONCLUSIONS
The reading distance and the pupillary diameter are the factors that most determine the amount of light potentially entering the eye. The calculated amount of short-wavelength radiation reaching the pupil is 1.4 times greater when using a smartphone than when using a PC-LED display. Children receive 40% more short wavelength light than adults when using the same device due to their anatomic conditions (shorter viewing distance) and higher accommodation abilities. When comparing reading on a tablet with reading on paper at a similar distance, blue light incidence is 7.5 times higher for the digital device.
REFERENCES
- Rosenfield M. (2011). Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic Physiol Opt. 31(5):502-515.
- Hue JE, Rosenfield M, Saa G. (2014). Reading from electronic devices versus hardcopy text. Work. 47(3):303-307.
- Nakamura S, Chichibu SF. (2000). Introduction to nitride semiconductor blue lasers and light emitting diodes: CRC Press.
- Nakamura S. (1997). Present performance of InGaN-based blue/green/yellow LEDs. Photonics West'97. International Society for Optics and Photonics.
- Ham W, Ruffolo J, Mueller H, Clarke A, Moon M. (1978). Histologic analysis of photochemical lesions produced in rhesus retina by short-wave-length light. Investigative ophthalmology & visual science. 17(10):1029-1035.
- Organisciak DT, Vaughan DK. (2010). Retinal light damage: mechanisms and protection. Prog Retin Eye Res. 29(2):113-134.
- Chamorro E, Bonnin-Arias C, Perez-Carrasco MJ, Munoz de Luna J, Vazquez D, Sanchez-Ramos C. (2013). Effects of light-emitting diode radiations on human retinal pigment epithelial cells in vitro. Photochem Photobiol.. 89(2):468-873.
- Yuodelis C, Hendrickson A. (1986). A qualitative and quantitative analysis of the human fovea during development. Vision Res. 26(6):847-855.
- Kaufman PL, Alm A. (2004). Adler fisiología del ojo: aplicación clínica: Elsevier.
- Winn B, Whitaker D, Elliott DB, Phillips NJ. (1994). Factors affecting light-adapted pupil size in normal human subjects. Investigat Ophthal Visual Sci. 35(3):1132-1137.
- Rosenfield M, Benzoni J. (2007). Amplitude of accommodation in children between 5 and 10 years of age. Investigat Ophthal Visual Sci. 48(13):975.
- Ovenseri-Ogbomo GO, Kudjawu EP, Kio FE, Abu EK. (2012). Investigation of amplitude of accommodation among Ghanaian school children. Clin Exp Optom. 95(2):187-191.
- Artigas J. (1995). Óptica Fisiológica: Psicofísica de la visión: McGraw-Hill/Interamericana de España.
- Klamm J, Tarnow KG. (2015). Computer Vision Syndrome: A Review of Literature. Medsurg Nurs. 24(2):89-93.
- Wethington H, Pan L, Sherry B. (2013). The Association of Screen Time, Television in the Bedroom, and Obesity Among School‐Aged Youth: 2007 National Survey of Children's Health. J Sch Health. 83(8):573-581.
- Winn B, Whitaker D, Elliott DB, Phillips NJ. (1994). Factors affecting light-adapted pupil size in normal human subjects. Invest Ophthalmol Vis Sci. 35(3):1132-1137.
- Yoshimura M, Kitazawa M, Maeda Y, Mimura M, Tsubota K, Kishimoto T. (2017). Smartphone viewing distance and sleep: an experimental study utilizing motion capture technology. Nat Sci Sleep. 9:59-65.
- Long J, Cheung R, Duong S, Paynter R, Asper L. (2017). Viewing distance and eyestrain symptoms with prolonged viewing of smartphones. Clin Exp Optom. 100(2):133-137.
- Argiles M, Cardona G, Perez-Cabre E, Perez-Magrane R, Morcego B, Gispets J. (2016). Real-Time Non-Intrusive Assessment of Viewing Distance during Computer Use. Optom Vis Sci. 93(12):1525-1531.
- Krigel A, Berdugo M, Picard E, Levy-Boukris R, Jaadane I, Jonet L, et al. (2016). Light-induced retinal damage using different light sources, protocols and rat strains reveals LED phototoxicity. Neuroscience. 339:296-307.
- Kim GH, Kim HI, Paik SS, Jung SW, Kang S, Kim IB. (2016). Functional and morphological evaluation of blue light-emitting diode-induced retinal degeneration in mice. Graefes Arch Clin Exp Ophthalmol. 254(4):705-716.
- Shang YM, Wang GS, Sliney D, Yang CH, Lee LL. (2014). White light-emitting diodes (LEDs) at domestic lighting levels and retinal injury in a rat model. Environ Health Perspect. 122(3):269-276.
- Jaadane I, Boulenguez P, Chahory S, Carre S, Savoldelli M, Jonet L, et al. (2015). Retinal damage induced by commercial light emitting diodes (LEDs). Free Radic Biol Med. 84:373-384.
- Lin CH, Wu MR, Li CH, Cheng HW, Huang SH, Tsai CH, et al. (2017). Editor's Highlight: Periodic Exposure to Smartphone-Mimic Low-Luminance Blue Light Induces Retina Damage Through Bcl-2/BAX-Dependent Apoptosis. Toxicol Sci. 157(1):196-210.
- Christensen R, Knezek G. (2017). Readiness for integrating mobile learning in the classroom: Challenges, preferences and possibilities. Computers Human Behav. 76(Supplement C):112-121.
- Chu C, Rosenfield M, Portello JK, Benzoni JA, Collier JD. (2011). A comparison of symptoms after viewing text on a computer screen and hardcopy. Ophthalmic Physiol Opt. 31(1):29-32.