2023: Volume 4, Issue 4
Past Issues
 Abstract
Abstract  PDF
PDFEndo- and Exoantigens and Development of Autoimmune Reaction
Trubitsyna IE*, Vorobyeva NN, Lesko KAM, Smirnov AV, Vinokurova LD
Loginov Department of Health of Moscow, Moscow Clinical Research Center named after A.S, Moscow, Russia
*Corresponding Author: Trubitsyna IE, Loginov Department of Health of Moscow, Moscow Clinical Research Center named after A.S, Moscow, Russia; Email: [email protected]
Received Date: September 5, 2023
Publication Date: September 19, 2023
Citation: Trubitsyna IE, et al. (2023). Endo- and Exoantigens and Development of Autoimmune Reaction. Clin Res. 4(4):18.
Copyright: Trubitsyna IE, et al. © (2023).
SUMMARY
The immunoinflammatory response is involved in the formation structural damage in organs with low immune resistance, but the stages of formation of this reaction are bad studied. In patients with acute and chronic pancreatitis alcohol etiology causes a reactive inflammatory reaction in the mucous membrane of the small intestine. Clarification of all stages of development of comorbidity forced to conduct experimental studies that were carried out on 45 white Wistar rats weighing 180-220 g under conditions mucous membrane (MM) of the stomach and duodenum. A feature of this study was that the animals were previously immunized according to the classical immunization schedule, with pancreatic homogenates (PG), different sections mucous membrane of the stomach (MM S) or duodenum (MM D). Rats were removed from the experiment on days 5, 10 and 20. Undoubtedly, the presence of damage to the pancreas promotes the development of an autoimmune reaction, in response to destruction and inflammatory response. Structural and functional damage to one’s own tissues occurs in other organs. The participation of several organs in a joint reaction depends from the immune tolerance of the organ to exo- and endoantigens. The presence of concomitant pathology it is not always possible to determine the “primary” organ that contributed to the formation of the autoimmune reaction. At the same, antibodies to endoantigens are formed from damaged tissues.
Keywords: endo- and exoantibodies, autoimmune reaction, pancreatitis, gastric and duodenal mucosa
INTRODUCTION
Immune System of the mucous membrane of the gastrointestinal tract (GIT) (MALT-system) constantly guards and ensures a safe transition "from the outside to the inside and from the inside to the outside". It is associated with the external environment, supports and regulates immune vital activity, is directly related to part of the immune system, plays a huge role in the successful functioning of the digestive tract and the whole organism [1]. A defect in the integrity of any barriers of the skin and mucous membranes leads to the penetration into the body of antigens from the outside (exoantigens I), which under normal conditions either do not enter or enter in a limited way. To strengthen the immune basis of the inflammatory process, we immunized animals according to the standard scheme using homogenates prepared at the rate of 1 g of tissue in 10 ml of saline. Animals were given 4 intraperitoneal injections of 2 ml of a homogenate containing 30 mg of protein per injection; injections were made 3 days later on the fourth. According to this scheme, antibodies are obtained in a titer of 1: 160–1: 640. The exoantigen (I) that has thus entered the body is absorbed by reticular cells, macrophages, and lymphocytes, which later turn into plasma cells that produce antibodies. The initial reaction between the antigen and the corresponding cells takes only a few minutes. At the first injection of the antigen (homogenate), a certain latent period is observed between the moment of injection of the exoantigen and the time of the appearance of antibodies in the blood of the object under study. The duration of the latent period depends on the properties and amount of the antigen, the method of its administration, the individual properties of the immunized. As a rule, the first antibodies are found in the blood of the animal 3-5 days after injection of I and reach the highest titer by 9-12 days. Following this, the antibody titer drops markedly. Taking into account these time periods, the dates of withdrawal of rats from the experiment on the 5th, 10th, and 17th days were chosen. Tissue damage was assessed using light microscopy. According to the literature, it is known that immune tolerance depends on local disorders, such as dysfunction of immunocompetent cells that do not produce antibodies enough, a violation of the concentration spectrum of different classes of immunoglobulins and changes in the formation and ratio of immune response mediators, which contributes to the development of neurogenic or immune inflammation [2], the concentration of pro-inflammatory mediators increases compared to control values, and the production of anti-inflammatory mediators is reduced. By the way, at the same time there should be a high sensitivity of peripheral tissues to inflammatory mediators [3]. It is conditionally possible to distinguish 4 groups of indicators that ensure the development of the autoimmune component: genetic, immunological, functional and specific, the presence of allergies. Under physiological conditions, the tone of the immune system, its systemic immune reactivity, is genetically programmed [3,4]. Local depends on the balanced production of regulatory cytokines that are part of the immune surveillance system [2-4]. They must be able or learn to recognize belonging to the body. Violation of cytokine concentration and their ratio plays a significant role in the chronicity and progression of diseases of the digestive system (DOD) [5-7]. The intensity of local and systemic autoimmune processes in pancreatic pathology depends on the response to its damage, accompanied by a change in the concentration of physiologically active compounds (PAS): cytokines (CK), neurotransmitters (5-HT Ach) responsible for the development and maintenance of immune and neurogenic inflammation (NI), for orientation in the material in our studies, divisions of antigens were introduced, terms were used - exoantigens that enter the body from the environment by inhalation, ingestion or injection, then their standard path they enter antigen-presenting cells. Endoantigens are produced by the cells of the body during the natural life of the tissue; upon cell death [8,9], cell fragments are presented on the surface of the lymphocyte (T-cell) in a complex with major histocompatibility complex type 1 (MHC I) proteins. At the same time, T cells secrete various toxins that cause the death of an infected or damaged cell. In order to prevent cytotoxic lymphocytes from killing healthy cells, autoreactive T-lymphocytes were limited in their presence in the extracellular matrix during the formation of immune tolerance and the reduction of the damaging effect against their own tissues in healthy cells. Simultaneously, T-lymphocytes differentiate and begin to play an important role in the acquired immune response. Ensuring the recognition and destruction of cells carrying foreign antigens, they enhance the effect of monocytes, natural (native) killer (NK-cells), and also take part in the conversion of IgM immunoglobulins to: IgGs. (IgG1, IgG2, IgG3, IgG4) IgA, IgE [5-8].
So, Purpose: in the conditions of the experiment, to trace the presence or not of immune inflammation in the GM and SOD in case of damage to the pancreas, to establish which organs of the gastrointestinal tract have low immune tolerance, combined with high immune reactivity of tissues [9].
MATERIAL AND METHODS
45 white rats of the Wistar line, weighing 180-220 g, were used. The content of animals in the vivarium corresponded to generally accepted sanitary rules. All experiments were carried out in accordance with the rules for the humane treatment of animals, regulated by Federal Law No. 498; other federal laws and other regulatory legal acts of the Russian Federation. During manipulations that caused pain, ether anesthesia was used. The animals were taken out of the experiment on the 5th, 10th, and 17th days. In acute pancreatitis up to 10 days, the release of the pancreas is impossible; it is “immured” in adipose tissue, forming one whole with it.
Immunization of animals, the spleen and thymus were weighed. The weight of the spleen ranged from 0.7 to 2 g. The average value was 1.35 g in the control, 0.995 g. The weight of the thymus increased by 50-60% in comparison with the control. After an external examination and selection of the biomaterial, a morphological study was performed - coolant, mucosa, pancreas.
Control for all groups - intact animals were used, which were injected with 2.0 ml of saline instead of homogenates (n=5). In the control groups of rats, no pathological changes in the gastric mucosa, mucosa, and prostate were detected, both visually and morphologically. The studied material - the tissue of the stomach (from the body and pyloric sections), duodenum and pancreas, was fixed in 10% neutral formalin, after histological wiring, embedded in paraffin, then the sections were stained with hematoxylin and eosin (h&e).
To identify digestive organs with low or high immune tolerance, a series of studies was conducted, in which the first group: intact animals that were injected with pancreatic homogenate, to establish the role of I (pancreatic homogenate) in the development of immune inflammation in the pancreas. Figure 1 shows a macropreparation of the pancreas after injection of the pancreas homogenate. The figure shows that the pancreas is edematous, with microcirculatory (MCC) disorders. The following is Figure 2, with micropreparations of the pancreas, inflammation with edema and a decrease in pancreatic tissue was revealed. Edematous fluid "spreads" the pancreatic lobules, disrupting blood flow, thereby contributing to the formation of necrosis. A distinctive feature of the inflammatory reaction after injection of I is a massive cellular infiltration of neutrophils, eosinophils, lymphocytes with the presence of plasma cells in the edematous fluid (Fig. 2 B. Pronounced cellular infiltrate in the lobules themselves. The ducts are dilated; the wall is destroyed in places, necrotic with the penetration of leukocytes into the lumen of the duct, a violation of the microcirculatory structure, plethora and small focal hemorrhages in the tissues of the lobules. There is no reaction in the coolant or SOD. In rats in the group of animals with damage to the mucosa, immune inflammation occurs on their own II in all parts of the mucosa or mucosa with the introduction of I coolant or SOD. Against the background of the existing damage, the CO caused an increase in the existing damage and the occurrence of additional damage to the CO in the marginal zone (Figure 3).
Homogenates of different sections of the GM or SOD injected into intact animals do not cause damage to the pancreas. PZH is not called.
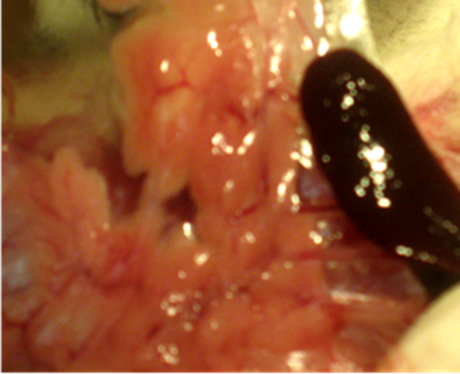
Figure 1: Pancreas after intraperitoneal administration of pancreatic homogenate according to the standard scheme, a macrophotograph of the pancreas.
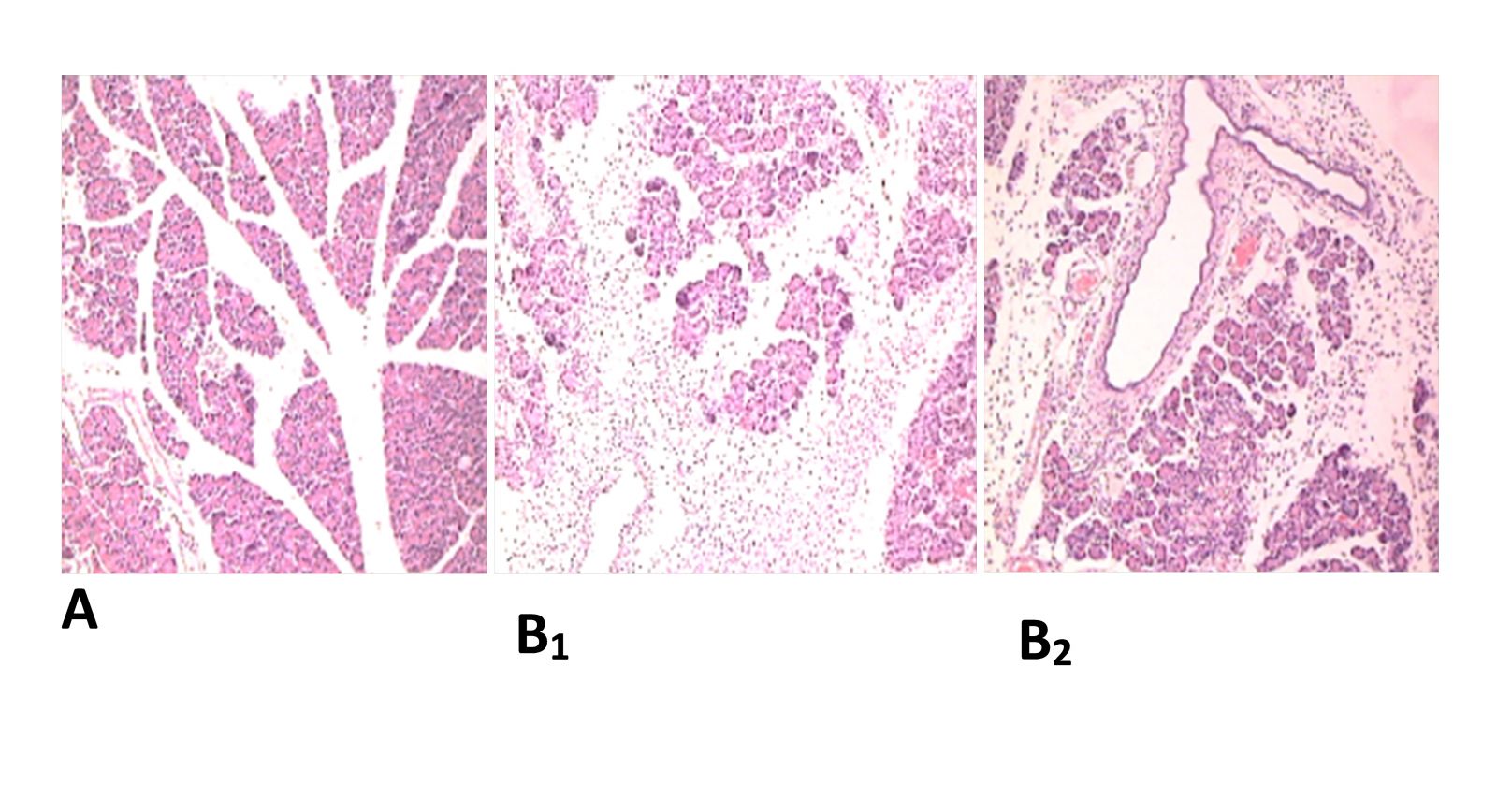
Figure 2: Pancreas. A. 1 hour after application of acetic acid application time 5 sec, edema and venous stasis, compression of acinar cells by edematous fluid h&e X180. B1,2 Pancreas. After the introduction of the pancreatic homogenate, the picture of inflammation with extensive edema and massive cell infiltration with neutrophils, eosinophils, lymphocytes, and plasma cells. There is cell infiltration in the lobules themselves, reduction of pancreatic tissue. Edematous fluid, "pushing" the pancreatic lobules, disrupts blood flow and causes tissue necrosis. The ducts are dilated, the wall is destroyed in places, anesthetized, abundant leukocyte infiltration of the wall with the penetration of leukocytes into the lumen of the duct. Small focal hemorrhages in the tissue of h&e lobules x240.
Figure 2 shows micropreparations of damage to the pancreas. A - damage by a chemical agent. B1,2 damage to the pancreas after immunization with homogenates of the pancreas tissue, in this case, I enters the experimental animals by intraperitoneal (ip), intraperitoneal (i/p) injection. So, in both cases, there is edema and a violation of the MCC, but after the introduction of I in the edematous fluid, the intercellular matrix, abundant cell infiltration, at the same time we noted that the ingestion of I into the body causes an increase in the mass of the spleen and thymus.
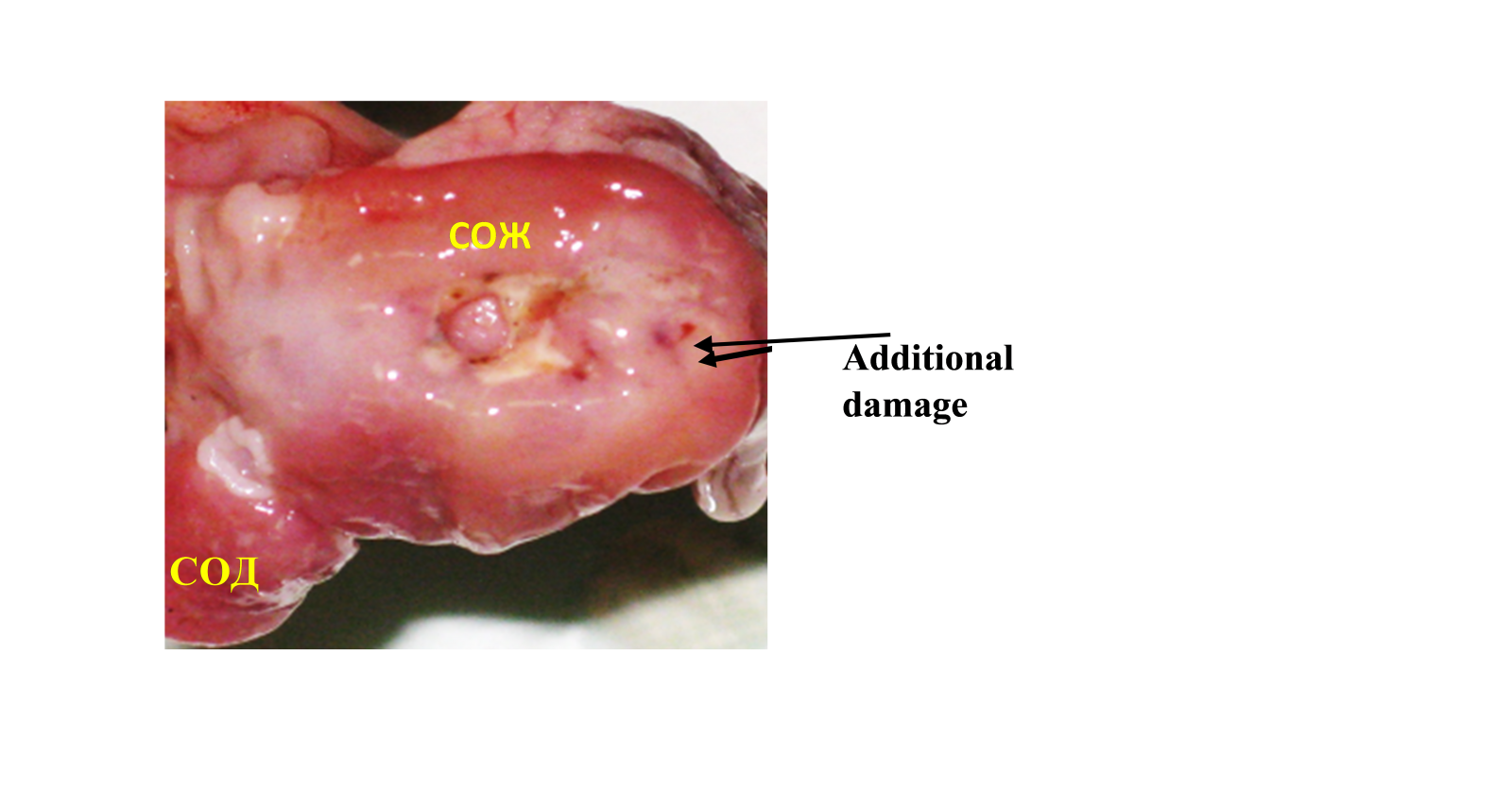
Figure 3: Macrophoto of ulcer gastric, gastric mucosa (GM) 5 days + intraperitoneal injection of gastric homogenate.
Experimental studies have revealed that the introduction of I from different organs has organ specificity, on the other hand, the introduction of I from different parts of the stomach, the CO reaction affects only the part whose homogenate was injected. The introduction of I SOD of the body of the stomach (TG), edema and hyperemia only in the area of the TG, SO of the pylorus in the pyloric region. Introduction of I, SOD homogenate - only in duodenal mucosa. It should be noted that with ulcerative lesions of the body of the stomach, there is a reaction of CO in the duodenum and other parts of the stomach (Figure 4).
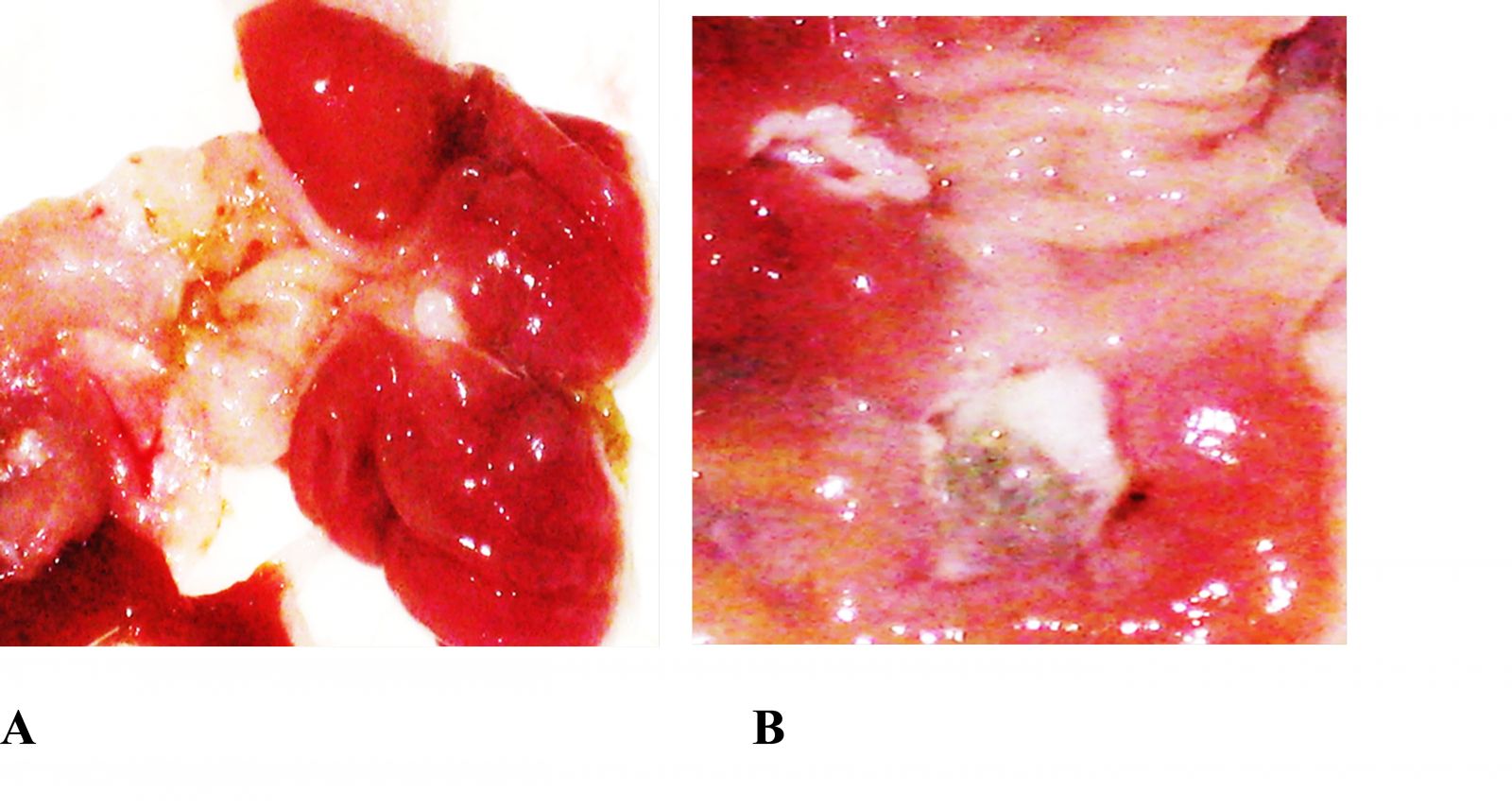
Figure 4: Endoantigens, acute phase of ulcerative lesions A. Acute duodenal ulcer, inflammatory reaction in (MD) SOD and (MG) gastric mucosa. B. Acute gastric ulcer, inflammatory reaction in (MG) gastric mucosa and (MD) SOD.
CONCLUSION
Summing up the data obtained in the experimental conditions, we can draw the following conclusions:
1. Pancreatic tissue does not respond to damage to the organs of the gastroduodenal zone. This indicates that the pancreas has low immune reactivity combined with high immune tolerance.
2. Coolant and SOD have low immune tolerance, with high tissue reactivity. This is confirmed by the fact that the presence of an acute injury in the pancreas is accompanied by immune inflammation in the GM and SOD. In contrast to the fact that acute damage to the GM and SOD does not affect the pancreas [13,14].
3. The conclusion is bold, but confirmed experimentally. Endoantigens (II) of the gastrointestinal mucosa do not have an individual effect on the organs, and on the departments of one organ, the entire SM reacts, regardless of the sections of the stomach. Acute damage (ulcer) to the gastric mucosa or SOD contributes to immune inflammation of the entire gastric mucosa of the duodenum. There is no differential effect. The introduction of I is specific: homogenate of CO from the body of the stomach causes a reaction in the CO of the body of the stomach, the introduction of homogenate of CO from the antrum only in the antrum of the CO of the stomach. SOD homogenate only in duodenal mucosa.
4. Prolongation of the immune inflammatory response occurs with repeated intravenous administration of homogenates. Or repeated damage to the coolant, mucosa or pancreas, but this requires a second operation, which is fraught with the death of the animal. It is easier to re-introduce homogenates.
REFERENCES
- Trubitsyna IE, Ruchkina IN, Mikhailova SF, Efremov LI, Degterev DA, Drozdova GA, et al. (2018). Malt-system of the mucous membrane of the gastrointestinal tract. Exp Clin Gastroenterol. 159(11):83-86
- Ado AD, Ishimova LM. (2000). Pathological Physiology.
- Khaitov RM, Ignatieva GA, Sidorovich IG. (2010). Immunology. Norm and Pathology.
- Chereshnev V, et al. (2012) Clinical Pathophysiology. St. Petersburg: SpetsLit.
- Troshin V. (2005). Heredity and health. Prevention and methods of treatment / Vladimir Troshin. –
- David PC. (2011). Microbes, genes and civilization / David P Clark. - Moscow: Higher School.
- Trubitsyna IE, Onishchenko NA, Lyundup AV, Knyazev OV, Gulyaev AS, Vasnev OS, et al. (2016). Immunomodulatory effect of allogeneic mesenchymal stem cells in rat bone marrow. Exp Clin Gastroenterol. 11(135):59-63.
- Trubitsyna IE, Chikunova BZ, Vorobyeva NN, Lagutina LD, Agafonov MV. (2011). Experimental studies as a method of comparative medicine. Gastroenterology of St. Petersburg.
- Trubitsyna I, Vinokurova L, Tarasova T, Lesko K, Dorofeev A, Papysheva L, et al. (2020). The Process of Formation the Autoimmune Reaction in the Gastric Mucosa the Damaged Liver. Gastroentero Hepatol Res. 14:001-007.
- Komarov FO, Galkin VA. Ivanov AI, Maksimov VA. (1983). Combined diseases of the organs of the duodenocholedochopancreatic zone.
- Harris TJ, Beck WC, Bhavaraju A, Davis B, Kimbrough MK, Jensen JC, et al. (2018). Severe acute gallstone pancreatitis with diffuse hemorrhagic gastritis. J Surg Case Rep. 2018(3):048.
- Yabuki K, Maekawa T, Satoh K, Tamasaki Y, Maekawa H, Kudoh K, et al. (2002). Extensive hemorrhagic erosive gastritis associated with acute pancreatitis is successfully treated with a somatostatin analogue. J Gastroenterol. 37(9):737-741.
- Back MS, Mok Yu M, Khan VS, Kim Yu S. (2014). A patient with eosinophilic gastroenteritis with acute pancreatitis and ascites. Intestinal liver. 8(2):224-227.
- Lankisch PG, Apte M, Banks PA. (2015). Acute pancreatitis. Lancet. 386(9988):85-96.