2023: Volume 4, Issue 3
Past Issues
 Abstract
Abstract  PDF
PDFSteroid-Sensitive Encephalopathy Associated With Autoimmune Thyroiditis (SREAT): Case Report
Diego Nicolas Guacaneme1,*, Claudio Alejando Jiménez Monsalve1, Orlando Oliveros Pasión2, Julieth Milena Rodríguez López3, Neiry María Zapa Pérez1, Hellen Kreinter3, Nelly Daniela Gonzalez Galvis2
1Neurology Department, Hospital Simón Bolívar, Bogotá, Colombia
2Emergency Department, Hospital Simón Bolívar, Bogotá, Colombia
3Neurology Resident, Universidad El Bosque, Bogotá Colombia
*Corresponding Author: Diego Nicolas Guacaneme Poveda, Neurology Department, Hospital Simón Bolívar, Bogotá, Colombia; Tel: +56 979634765; Email: [email protected]
Received Date: June 8, 2023
Publication Date: August 05, 2023
Citation: Guacaneme DN, et al. (2023). Steroid-Sensitive Encephalopathy Associated With Autoimmune Thyroiditis (SREAT): Case Report. Clin Res. 4(3):17.
Copyright: Guacaneme DN, et al. © (2023).
ABSTRACT
Background: Steroid-responsive Encephalopathy Associated with Autoimmune Thyroiditis (SREAT) is a rare, controversial and underdiagnosed entity characterized by an acute or subacute onset of encephalopathy. It is a diagnosis of exclusion with supporting criteria that include high titers of anti-thyroid antibodies, a history of Hashimoto's thyroiditis, and a good response to steroids. Case report: An 18-year-old female patient with hypothyroidism and episode of change in behavior, hallucinations and episodes of generalized tonic-clonic movements, normal skull tomography, cerebrospinal fluid with pleocytosis without signs of infection and positive anti-thyroid antibodies with adequate response to management with steroids Conclusion: We considered SERAT as an entity that needs to be rediscovered as it has conflicting results that question if it is a syndrome or a myth. The literature is especially lacking in Colombia where there are not many published cases.
Keywords: Autoimmune encephalopathy, thyroiditis, Hashimoto's encephalopathy, anti-thyroid antibodies, case report
INTRODUCTION
Steroid-responsive encephalitis associated with autoimmune thyroiditis (SREAT) is a rare and controversial entity due to its clinical course and symptoms [1]. It was first described in 1966 as Hashimoto's Encephalitis (HE) but the name was changed because not all patients had hypothyroidism, there was a lack of knowledge of the pathophysiology and the response to steroids was remarkable [2]. Clinically it is characterized by neuropsychiatric symptoms with behavioral changes, cognitive impairment, tremors, myoclonus, gait disturbances, sleep disorder, stroke-like episodes and seizures [3,4]. This entity is associated with the presence of anti-TPO (anti-thyroid peroxidase) and anti-TG (anti-thyroglobulin antibodies) antibodies in serum or CSF. For the diagnosis there must not be any other clear etiology including absence of immune mediated disorders with well-characterized neuronal antibodies in serum and CSF [1-2,4].
To our knowledge there are only two reported cases of patients with this entity in Colombia [5,6]. We describe the case of a young patient with hypothyroidism and encephalopathy with positive anti-thyroid antibodies and a favorable response to immunotherapy.
CASE
An 18-year-old female was brought to the emergency department by her family because of concerns about behavioral changes. She had been in his usual until 20 days before this presentation when insomnia developed followed by delusions of religious content, visual and auditory hallucinations and a suicide attempt. She was admitted initially in another hospital with a psychiatric unit where a diagnosis of a first acute psychotic episode was made. After having three generalized tonic-clonic seizures she was referred for neurologic evaluation. Her past medical history was positive for a diagnosis of hypothyroidism associated with Hashimoto's thyroiditis at eleven years of age. She was on treatment with levothyroxine 150 mcg per day.
On admission, the patient was disoriented, with non-fluent aphasia and disorganized speech. Stiffness and fragmented movements were seen predominantly in the upper limbs. Stretch reflexes were hyperactive and symmetric with bilateral Aquilian clonus. Subsequently, the patient had progressive deterioration with stupor requiring orotracheal intubation and management in the intensive care unit.
A cerebral MRI showed no alterations in the brain parenchyma nor abnormal enhancements. Lymphocytic pleocytosis of 57 cells/ mm3 was observed in the cerebrospinal fluid (CSF), with a negative result of the Polymerase Chain Reaction (PCR) assay for herpes simplex virus.
After excluding an infectious etiology and while awaiting the results of anti-NMDA and anti-thyroid antibodies it was decided to start therapy with methylprednisolone rapidly followed by immunoglobulin, achieving neurological and clinical improvement.
Anti-TG and anti TPO antibodies were both positive in 2886 IU/ml and > 20,000 respectively. Other complementary studies were: antinuclear antibodies (ANAS) with a granular pattern and a value of 1:160 and normal thoracic and abdominal CT scans with gadolinium. The follow-up laboratories of antithyroid antibodies showed a progressive decrease until a complete normalization.
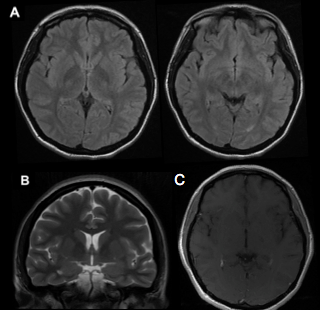
Figure: (A) Axial T2-weighted sequence brain MRI with attenuated fluid inversion recovery (FLAIR) without alterations in cerebral parenchyma (B) Coronal T2-weighted sequence without alterations (C) Axial T1-weighted sequence with contrast rules out abnormal enhancements.
DISCUSSION
Our patient is a young woman with a subacute onset of behavioral changes, epilepsy and altered consciousness and a history of Hashimoto thyroid disease. She had positive anti-thyroid antibodies, and exhibited a great improvement with steroids.
SREAT is not a frequently described entity which makes the diagnosis a challenge with some reported cases having even a delay of decades from the onset of symptoms to treatment [7].
SREAT has an estimated prevalence of 2.1 per population of 100,000. There is a female preponderance with cases being reported in patients aged 14 to 70 years (average age of onset 40 to 55 years) [8]. Laboratory findings are not specific, with some patients exhibiting an increase in inflammatory markers such as elevated transaminases in approximately 38% to 50% of the cases [8]. Usually, neuroimaging studies are normal or have non-significant changes [1,2,8].
Although anti-TG and anti-TPO antibodies are part of the diagnostic criteria, they do not explain the pathogenesis of the disease and they can be elevated in 13% of healthy people [1]. Matozzi, et al found a similar rate of TPO antibodies in both cases (patients with HE) and controls showing poor specificity of the test. There is also no clinical correlation between their values and the severity of the symptoms and the majority of the patients are euthyroid. [1,2,9,]
Treatment of Hashimoto's encephalopathy has two goals. The first is to control the autoimmune process with the administration of immune modulators or plasma exchange. The second thing is to control the complications of the disease: in the case of seizures, add anti-epileptics [10]. The delay in starting treatment is associated with worse prognosis [11].
Classically first-line treatment consists of high doses of steroids that can be administered intravenously or orally followed sometimes by a maintenance dose (intravenous methylprednisolone, 500-1,000 mg/day, for 5 days and continue with oral prednisone 1-2 mg/kg/day) [2,9,12]. The maintenance dose can last from months to one or two years [10].
Most patients improve completely after the onset of corticotherapy, but the possibility of relapse may be as high as 12.5%-40% [13].
Intravenous immunoglobulin is useful when patients have an incomplete response to steroids, or when relapses occur at the time of de-escalation. In the case of monoclonal antibodies, the suggested dose of rituximab is 1000 milligrams intravenously on days one and 14; and then once every six to nine months, depending on the leukocyte count [10].
Second line treatment includes immunosuppressive drugs such as azathioprine, cyclophosphamide and methotrexate. [1,2,9,14].
Plasma exchange has been shown to remove anti-thyroid peroxidase (anti-TPO) antibodies. However, no improvement in clinical or neurophysiological parameters has been observed, despite significant reductions in anti-TPO antibodies [10].
Sequelae include cognitive impairment, and recurrent refractory seizures are more common in children [10].
The writing of the case is very objective and direct, however, the study is limited.
CONCLUSION
We considered SERAT as an entity that needs to be rediscovered as it has conflicting results that question if it is a syndrome or a myth [12]. The literature is especially lacking there are not many published cases. Efforts should be done to better characterize a group of patients with a subacute onset of encephalopathy, possibly immune mediated that may benefit from early therapy with steroids.
FUNDING
The work was done with our own resources, in addition to the volunteer work of the researchers.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest
CONTRIBUTIONS
All authors contributed to the preparation of the material, the compilation of the patient's medical history data, as well as the writing of the manuscript. All authors approved the final manuscript.
ETHICS DECLARATIONS
Ethical Approval
The local ethics committee of the institution approved the study, which has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Informed Consent
The patient gave informed consent prior to inclusion in the study.
REFERENCES
- Castillo P, Woodruff B, Caselli R, Vernino S, Lucchinetti C, Swanson J, et al. (2006). Steroid-responsive encephalopathy associated with autoimmune thyroiditis. Arch Neurol. 63(2):197-202.
- Graus F, Titulaer MJ, Balu R, Benseler S, Bien CG, Cellucci T, et al. (2016). A clinical approach to the diagnosis of autoimmune encephalitis. Lancet Neurol. 15(4):391-404.
- Endres D, Perlov E, Stich O, Tebartz L. (2016). Steroid responsive encephalopathy associated with autoimmune thyroiditis (SREAT) presenting as significant depression. BMC Psychiatry. 16:184.
- Chong JY, Rowland LP, Utiger RD. (2003). Hashimoto encephalopathy: syndrome or myth? Arch Neurol. 60:164-171.
- Contreras AS, Rojas SA, Manosalva A, Méndez PA, Lorenzana P, Restrepo JF, et al. (2004). Hashimoto encephalopathy (autoimmune encephalitis). J Clin Rheumato. 10(6):339-343.
- Mantilla SE. Guerrero A, Montoya LE, Giraldo K, Aguirre HE. (2018). Encefalopatía de Hashimoto: reporte de caso y revisión de la literatura. Neurología Argentina. 11(3):177-180.
- Tjong E, Gardner R, Peng Y. (2019). SREAT presenting as decades of intractable seizures and isolated delusional episodes with clinical, laboratory, and EEG confirmation of treatment response. SAGE Open Med Case Rep. 7:1-8.
- Laurent C, Capron J, Quillerou B et al. (2016). Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT): Characteristics, treatment and outcome in 251 cases from the literature. Autoimmun Rev. 15(12):1129-1133.
- Liyanage CK, Munasinghe TMJ, Paramanantham A. (2017). Steroid-Responsive Encephalopathy Associated with Autoimmune Thyroiditis Presenting with Fever and Confusion. Case Rep Neurol Med. 2017:1-4.
- Pinedo-Torres I, Paz-Ibarra JL. (2018). Current knowledge on Hashimoto's encephalopathy: a literature review. Med Wave. 18(6):e7298.
- Salvador E, Guerrero A, Montoya L, Giraldo K, Aguirre H. (2018). Hashimoto's encephalopathy case report literature review.
- Collao-Parra JP, Romero-Urra C, Delgado-Derio C. (2018). Encefalitis autoinmunes: criterios diagnósticos y pautas terapéuticas. A review. Rev Med Chil. 146(3):351-361.
- Maryam J, Shafaq S, Ali S, Mohammad W. (2021). Hashimoto’s Encephalopathy: A Remediable Cause of Unexplained Encephalopathy. J Clin Stud Med Case Rep.
- Zhou JY. Lopes J, Blamoun J, Li L. (2016). Hashimoto encephalopathy: literature review. Acta Neurol Scand. 135(3):285-290.