2023: Volume 4, Issue 2
Past Issues
 Abstract
Abstract  PDF
PDFThe Spread of Covid-19 and International Students’ Intention to Leave China: A Self-Determination Perspective
Bernard Gumah1,2*
1Kwame Nkrumah University of Science and Technology (KNUST), Department of History and Political Studies
2National Identification Authority (NIA) M680 Ministries Accra
*Corresponding Author: Bernard Gumah, Kwame Nkrumah University of Science and Technology-Kumasi, Ghana; Email: [email protected]
Received Date: April 14, 2023
Publication Date: May 15, 2023
Manuscript Number: MG_P00239
Citation: Gumah B. (2023). The Spread of Covid-19 and International Students’ Intention to Leave China: A Self-Determination Perspective. Clin Res. 4(2):12.
Copyright: Gumah B. © (2023).
ABSTRACT
Self-determination refers to the competence to think independently and autonomously make choices, which contributes to the individual’s desire for absolute control based on three basic psychological needs (autonomy, competence, and relatedness). The study aimed to establish the influence of self-determination on international students’ intention to leave China due to the spread of COVID-19. Using 553 international students who participated in two rounds of data collection, regression analysis showed that rather than the region where an international student originates, the province of residence in China influences the intention to leave China. Also, self-determination mediates the effect of the province of origin and the intention to leave China. The reason could be the infection rate in individual provinces and the controlling nature of the measures instituted to combat the spread of the virus. We show the implication and contribution to the theory of self-determination.
Keywords: Self-determination; basic psychological needs; COVID-19; international students; intention to leave
INTRODUCTION
Studies show how satisfying the three psychological needs (autonomy, competence, and relatedness) aids adjustment and adaptation to new conditions (Houlfort et al., 2015; Philippe & Vallerand, 2008; Vansteenkiste, Lens, Soenens & Luyckx, 2006) [1-3]. We, therefore, use the three psychological needs in the self-determination theory to explain factors that influence individual adjustment and adaptation during emergencies like COVID-19.
The emergence of COVID-19, a public health catastrophe, has affected people’s lives worldwide. In this critical state of a public health emergency, people prefer to be where they perceive to be safe or adopt behaviors perceived to be safe. Health-related behaviors may not be inherently interesting or enjoyable and are unlikely to be felt as intrinsically motivated. However, health-related behaviors will result in significant outcomes to the individual and are central to their self-worth. This has potentially significant ramifications for motivating individuals to engage in healthy behaviors. Restrictive measures aimed at limiting the spread of COVID-19 disrupted people’s work routine and life and may interfere with what individuals perceive as healthy behaviors. For instance, many people may have to stop working or work from home, which in turn may impact their health and well-being (Zhang, Wang, Rauch, & Wei, 2020) [4]. The psychosocial effect associated with drastic lifestyle changes of at-risk communities is sometimes primarily ignored, as is evident in the Ebola-affected regions. Moreover, the mental health needs of confirmed patients, their families, medical staff, or the general population received little attention (Bitanihirwe, 2016) [5].
There are no known studies on coping strategies of individuals, particularly how psychological need satisfaction is relevant for infected and uninfected individuals to cope while in foreign countries in the time of a pandemic. Specifically, there is no study on COVID-19 and international students’ intention to leave. Since COVID-19 is a recent occurrence, it is worth exploiting as a medical phenomenon with a psychosocial effect. Studies are currently mainly in epidemiology, clinical characteristics, outcomes, and treatment of confirmed cases infected with 2019-nCoV (Huang et al., 2020) [6] and digital marketing (Clement Addo, Fang, Asare, & Kulbo, 2021) [7].
Coronaviruses (Coronaviridae) are non-segmented positive-sense RNA viruses belonging to the Coronaviridae family under the order Nidovirales (Drosten et al., 2003; Ksiazek et al., 2003) [8,9]. Earlier versions of the Coronaviridae virus include but not limited to severe acute respiratory syndrome coronavirus (SARS-CoV) (Drosten et al., 2003) [8] and what was known as the Middle East respiratory syndrome coronavirus (MERS-CoV) (Zaki, Van Boheemen, Bestebroer, Osterhaus, & Fouchier, 2012) [10]. Even though these viruses are known to have existed among animals, most human coronavirus infections are relatively mild. The previous versions claimed more than 1000 lives out of the 10000 cases recorded, and China recorded the highest fatalities. China seems to be fertile ground for the nCoV family (WHO, 2004) [11]. Based on the symptoms and the laboratory test results, the unknown virus, first detected in December 2019, was initially identified as the 2019 novel coronavirus (2019-nCoV) (Huang et al., 2020) [6]. The disease has been renamed “coronavirus disease 2019” (abbreviated “COVID-19”) (World Health Organization, 2020a).
The World Health Organization’s (WHO) International Health Regulations Emergency Committee on 30 January, 2020, acknowledged the outbreak as a “public health emergency of international concern” (PHEIC). Representatives of the Ministry of Health of the People’s Republic of China reported 7711 confirmed and 12167 suspected cases. Of the confirmed cases, 1370 were severe, 124 recoveries, and 170 deaths. The WHO Secretariat reported 83 cases in 18 countries. On 11th March, WHO reported 118,000 cases in 114 countries, with 4,291 lives lost; consequently, they declared COVID-19 a pandemic (World Health Organization, 2020a) [12]. There was a drastic decline in new infections in China, and Europe became the epicenter. The trend in the spread of the virus demanded health-related behaviors to limited the spread. However, these health-related behaviors may interfere with individuals’ desire for self-determination as a means of taking action voluntarily.
Self-determination Theory (SDT)
Self-determination theory (SDT), as an aspect of social psychology, focuses on the influence of the social environment on values, attitudes, motivations, and behaviors. According to Catalano et al. (2004, p. 19) [13], self-determination is “the ability to think for oneself and to take actions consistent with that thought.” It refers to competence in thinking for oneself and autonomy in making choices. Self-determined people can make choices according to their thinking and are less likely to submit to outside pressure. This is based on the view that humans are inherently active, intrinsically motivated, and oriented toward naturally developing through integrative processes. These processes operate effectively toward healthy development and psychological well-being, which are nutrients needed for both biological and psychological development (Ryan, 1995) [14]. Without these nutrients, these natural processes will be impaired, resulting in experiences, development, and less than optimal behaviors. SDT research Initially focused on intrinsic motivation. Subsequently, the internalization of extrinsically motivated activities was addressed (Ryan & Connell, 1989) [15].
Internalization reflects how individuals truly integrate or take in ambient values or practices. To fully internalize an activity that is not interesting, a person must value and experience ownership of that behavior (Ryan & Deci, 2017) [16]. Internalization requires competence and the satisfaction of autonomy. The inclusion of relatedness was because of the realization that a genuine sense of connection to others was necessary to encourage the pursuit of particular activities and goals. Competence, autonomy, and relatedness are the three psychological needs (Deci & Ryan, 2015) [17]. The three psychological needs must be satisfied to trigger internalization, while the absence of one hampers internalization (Milyavskaya, Nadolny, & Koestner, 2014) [18].
The basic psychological needs theory (BPNT) is one of the six mini-theories within the SDT. BPNT was to account for the effects associated with satisfaction of autonomy, competence, and relatedness. Psychological needs are defined in a narrow and more specific as psychological nutrients that are vital for individuals’ growth, adjustment, and integrity (Ryan, 1995) [14] .According to the BPNT, competence, autonomy, and relatedness are essential for optimum functioning and development. They are also crucial for basic needs, satisfaction for well-being and a mediator of the effects of social contexts on wellness. Ng et al. (2012) [19] view need support as a precursor of health outcomes and behavior change and an intervener and moderator of health outcomes and behavior change. It is also a method for initiating, improving, and sustaining health outcomes and behavior change. Baard et al. (2004) [20] need satisfaction between person-level has predicted better performance and better psychological health in the workplace. At the within-person level, general need satisfaction was associated with greater psychological health at the personal level. Daily, people experienced more significant positive effects and less negative effects on those days when they got more satisfaction with their basic needs (Reis, Sheldon, Gable, Roscoe, & Ryan, 2000) [21]. We identified studies of the basic need for autonomy, relatedness, and competence in various domains, contexts, and cultures (Ng et al., 2012; Niemiec & Ryan, 2009; see Rigby & Ryan, 2018; Vansteenkiste et al., 2006) [3,19,22,23].
Autonomy is the experience of volition and willingness, which results in a sense of integrity resulting from authentic self-endorsement of one’s actions, thoughts, and feelings (Ryan & Deci, 2000) [24]. Autonomy support refers to “the interpersonal sentiment and behavior one person provides to identify, nurture, and develop the other’s inner motivational resources – such as the need for autonomy, intrinsic motivation, personal interests, intrinsic goals, and self-endorsed values” (Su & Reeve, 2011, p. 160) [25]. Where autonomy is frustrated, it results in a feeling of being pushed in an undesirable direction. Autonomy-supportive strategies include providing a meaningful rationale for change and avoiding controlling language that may convey pressure, control, or guilt. Providing choice and the adoption of alternatives, and facilitating the setting of autonomous, personally relevant goals or outcomes (Teixeira, Silva, & Marques, 2016) [26].
The feeling of care, warmth, and bonding, satisfied by connecting to and feeling significant to others, is relatedness (Beachboard, Beachboard, Li, & Adkison, 2011) [27]. Given the importance of interpersonal support in promoting behavior change, supporting the need for relatedness is vital to ensure individuals in need of change have sufficient trust and rapport with those who support them to assimilate messages (Hagger & Protogerou, 2020) [28]. When relatedness is not satisfied, it leads to loneliness, social exclusion, and alienation. Relatedness support can be enabled through the appreciation and respect for others’ perspectives, recognizing and expressing understanding of negative emotions and conflict, and engaging in reflective listening (Teixeira et al., 2016) [26].
Competence refers to the feeling of a sense of mastery and effectiveness. A person becomes satisfied when engaging in activities and experiences that require such skills and expertise. If competence is frustrated, it results in helplessness and failure (Vansteenkiste, Ryan, & Soenens, 2020) [29]. Competence-supportive actions include first identifying barriers to change and suggesting ways to overcome them. Secondly, setting goals that are optimally challenging, realistic, and have meaningful outcomes. Thirdly, tailoring strategies and goals to peoples’ skills and offering clear and constructive informational feedback about goal progress.
Although a high level of competence is necessary, it is insufficient for health behavior adoption or treatment adherence; an increased sense of volition and autonomy must also be present (Ryan, Patrick, Deci, & Williams, 2008) [30]. The absence of one of these basic needs frustrates the process of internalization. For instance, bonding with others and feeling capable of carrying out boring activities may be the beginning of internalization. The internalization process will only be partial without the need for autonomy. Without autonomy, people may engage in activities after approval or please others and avoid guilt (Haerens, Aelterman, Vansteenkiste, Soenens, & Van Petegem, 2015) [31]. Research shows that satisfying the three basic needs is critical for wellness, both situationally (Reis et al., 2000) [21] and developmentally (Grolnick, Ryan, & Deci, 1991) [32]. In the view of Kluwer et al. (2020) [33], the three needs, each uniquely but interactively, are indispensable for people’s well-being across cultures, contexts, and age groups. Also, Ryan and Deci (2017) [16] argue for the importance of these needs on deductive grounds, specifically for integration, coherence, and adaptation where necessary.
Undeniably, maintaining a healthy lifestyle is affected by ongoing need satisfaction and frustrations (Ng et al., 2012) [19]. Besides, the crucial role of these basic psychological needs is demonstrated in the possible costs of their frustration, which predicts lower happiness and multiple forms of maladjustment (Bartholomew et al., 2018) [34]. BPNT recognizes that specific human factors foster psychological growth and proactivity. Indeed, no fully functioning person for whom relatedness, autonomy, and competence needs are unimportant. If psychological needs are intrinsic, they should be universally applicable and operative (Ryan & Deci, 2017) [16] and thus pertinent for individuals regardless of their cultural background (Benita, Benish-Weisman, Matos, & Torres, 2020) [35], demographic characteristics (Henning et al., 2019) [36], and personality (Mabbe, Soenens, Vansteenkiste, & Van Leeuwen, 2016) [37]. We, therefore, propose the following hypotheses;
Hypothesis 1: Region of origin is positively associated with international students’ self-determination to adjust to the conditions related to the spread of COVID-19.
Hypothesis 2: A foreigner’s location in China is positively associated with the self-determination to adjust to conditions related to the spread of COVID-19.
Hypothesis 3: Region of origin is positively associated with international students’ intention to leave China.
Hypothesis 4: The province of residence in China is positively associated with international students’ intention to leave China.
Hypothesis 5: Foreigners’ self-determination is positively associated with international students’ intention to leave China.
Hypothesis 6: The level of a foreigner’s self-determination positively mediates the relationship between the region of origin and the desire to leave China.
Hypothesis 7: The level of a foreigner’s self-determination positively mediates the relationship between the province of residence in China and the desire to leave China.
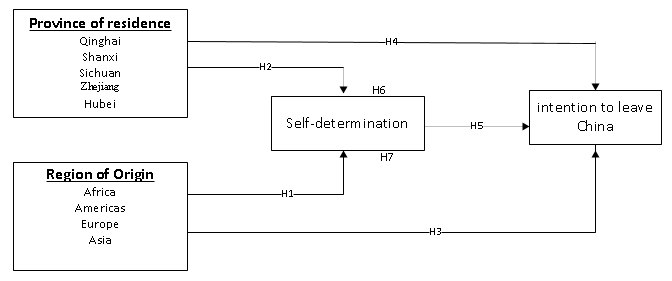
Figure 1: Theoretical model
METHOD
Participants
Our sample population is international students in China. We collected the data in two phases. The first data were collected from January to February when the infection rate was high and the disease was considered an epidemic in China (World Health Organization, 2020b) [38]. The second set of data was collected from March to April when the disease was spreading to other countries and subsequently declared a pandemic by the WHO (World Health Organization, 2020a) [12]. We introduced the questionnaires and circulated them on online platforms exclusively for international students. A total of 803 and 611 international students participated in the first and second rounds of data collection, respectively. The Mac address of the participant’s device was registered and used to identify those who participated in the first and second rounds. Based on this, a total of 553 participated in both rounds of data collection. We, however, acknowledge that participants could use different devices to access the questionnaire. Such participants were considered other respondents since linking them to the first data is impossible. We included a question on the current location of participants to eliminate those that had already left China during the second data collection phase.
Table 1 shows the participants’ background information whose participation in the first and second round of data collection was confirmed. Of the 553 participants, 365 were from the African region, and 271 were residents of the Sichuan province. There were 324 males, with married participants being 326 and 313 in the age group 26 to 35.
Table 1: Background information of respondents (n=553)
|
Variable |
Label |
Frequency |
% |
|
Gender |
Female |
229 |
41.5 |
|
Male |
324 |
58.5 |
|
|
Age |
Below 25 |
115 |
20.8 |
|
26-35 |
313 |
56.6 |
|
|
36-45 |
125 |
22.6 |
|
|
Marital status |
Single |
227 |
41.1 |
|
Married |
326 |
58.9 |
|
|
Educational Level |
Bachelor |
81 |
15.1 |
|
Masters |
325 |
58.7 |
|
|
Ph.D |
104 |
18.8 |
|
|
Others |
43 |
7.7 |
|
|
Field of study |
Humanities/Social Sciences |
21 |
3.8 |
|
Business |
156 |
28.3 |
|
|
Engineering |
146 |
26.4 |
|
|
Sciences |
229 |
41.5 |
|
|
Scholarship status |
Full School Scholarship |
213 |
38.5 |
|
Chinese govt Scholarship |
165 |
29.8 |
|
|
Partial scholarship |
123 |
22.2 |
|
|
Self-funding |
52 |
9.4 |
|
|
Region of Origin |
Africa |
365 |
66.0 |
|
Americas |
84 |
15.1 |
|
|
Europe |
63 |
11.3 |
|
|
Asia |
41 |
7.5 |
|
|
Province of residence |
Qinghai |
21 |
3.8 |
|
Shanxi |
52 |
9.4 |
|
|
Sichuan |
271 |
49.1 |
|
|
Jiangsu |
31 |
5.7 |
|
|
Zhejiang |
62 |
11.3 |
|
|
Hubei |
115 |
20.8 |
MEASURES
Self-determination is measured using a 5-point Likert scale from (1) strongly disagree to (5) strongly agree. We adopted the work needs satisfaction scale (WNSS) (Autin et al., 2019) [39] and modified it to fit the context of COVID-19. The 9 item scale shows an acceptable Cronbach Alpha of .795. Statements such as I feel connected to other people who have been affected by the restrictions imposed due to COVID-19 (relatedness), I take decisions autonomously without anyone questioning or restricting me (autonomy), I feel good about my ability to take part in informing others about COVID-19 within my immediate environment (competence).
Region of origin was measured by dividing various parts of the world into four regions: Africa, the Americas, Europe, and Asia. Based on current infections in the rest of the world, we ordered the region of origin from the lowest infection rate to the highest infection rate (see World Health Organization, 2020b) [38]. Similarly, we also used the 23 provinces and administrative regions in China as the location of each participant. Respondents came from 6 provinces. Provinces were ranked based on infection rate as of 15 March 2020, from the lowest (1) Qinghai to (6) Hubei. We assume that the magnitude of the intensity of COVID-19 suspected and confirmed cases in a province determines the measures authorities will implement to reduce the spread of the disease. These are contextual factors that could influence the satisfaction of basic needs.
We included a question on whether respondents intend to go back to their home countries and return later after the control of COVID-19. We used a modified version of the 3-item intent to leave scale by Weisberg (1994) [40]. Respondents were required to indicate their level of agreement with a statement using a Likert scale from (1) strongly disagree to (5) strongly agree. Sample statements include Since the epidemic started, I often think of leaving China, In the past weeks, I have been actively looking for an opportunity to leave China. A higher value indicates a higher intention to leave. The Cronbach alpha for this scale was 0.83.
Since our study population is foreign students, we control for education, scholarship status, the field of study, age, marital status, gender, and level of education. Knowing the number of cases in a province could cause fear and trigger a desire to leave, and we included the infection rate as a control variable.
RESULTS
The correlation in Table 2 indicates a negative correlation between self-determination and province of residence (β=-.111, p<.05) and a positive correlation with the region of origin (β=.021, p<.05). Also, self-determination correlates negatively with the intention to leave China (β=-.451, p<.05). We also show how other personal characteristics like gender correlates with the intention to leave China during the outbreak of COVID-19. Based on the recommendation of Baron and Kenny (1986) [41], we satisfied the conditions for conducting a mediation analysis.
Table 2: Partial correlation of variables.
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
|
1 |
1 |
|
|
|
|
|
|
|
|
|
|
2 |
-.132 |
1 |
|
|
|
|
|
|
|
|
|
3 |
-.018 |
-.214 |
1 |
|
|
|
|
|
|
|
|
4 |
.134 |
.165 |
-.375 |
1 |
|
|
|
|
|
|
|
5 |
.215** |
.106 |
.222 |
.036 |
1 |
|
|
|
|
|
|
6 |
.287 |
-.334 |
.052 |
.064 |
.111 |
1 |
|
|
|
|
|
7 |
-.252 |
.145 |
-.358* |
-.003 |
.468** |
.209 |
1 |
|
|
|
|
8 |
-.306 |
.061 |
-.248 |
.086 |
.406* |
.457** |
.298 |
1 |
|
|
|
9 |
.021** |
-.111** |
.031 |
.034 |
.355* |
.235 |
.401* |
.014 |
1 |
|
|
10 |
.100** |
-.092** |
.504** |
-.059 |
.062 |
-.240 |
-.128 |
-.451** |
.056 |
1 |
|
M |
1.86 |
6.00 |
1.56 |
2.05 |
1.85 |
2.27 |
3.05 |
3.41 |
3.70 |
1.41 |
|
SD |
1.167 |
3.101 |
.503 |
.653 |
.655 |
.827 |
.950 |
.503 |
.632 |
.503 |
1=Region of origin, 2=Province of residence, 3=Gender, 4=Age range, 5=marital status, 6=Level of education, 7=field of study, 8=Scholarship status, 9=Self-determination, 10=Intention to leave
Table 3 shows the level of self-determination for the two periods. We determined the level of self-determination by using the means of the scales used to measure self-determination. Means less than 3.0 are considered low, 3.0 to 3.9 is medium, while 4-5 represents high self-determination. Generally, there was a higher level (49.0%) of self-determination in the first data collection period. In the second phase, 47.6% had medium self-determination, showing a reduction in the level of self-determination. There was also an increase in the number of international students with the intention to leave China in the second phase of data collection.
Table 3: Level of self-determination of participants
|
|
Round 1 (n=803) |
Round 2 (n=611) |
|||
|
Frequency |
% |
Frequency |
% |
||
|
High Self-determination |
393 |
49.0 |
194 |
31.7 |
|
|
Medium self-determination |
257 |
32.1 |
291 |
47.6 |
|
|
Low self-determination |
152 |
18.9 |
126 |
20.6 |
|
|
Intent to leave |
Agree |
424 |
52.8 |
208 |
34.0 |
|
Neutral |
167 |
20.8 |
23 |
3.8 |
|
|
Disagree |
212 |
26.4 |
380 |
62.2 |
|
We conducted a linear regression analysis to establish the direct effect of the independent variables on the mediator, as presented in table 4. Since the independent variable is categorical, we used the effect coding method in this analysis. In using effect coding, we first satisfied the conditions for using this coding method. First, the errors are independently and normally distributed. Secondly, all group means must lie on a straight line and the errors should not correlate with the independent variable. Effect coding is applied when groups are compared rather than with a reference group (Koslowsky, 1988) [42]. The analysis shows a direct effect of the independent variables on the mediator, allowing us to accept hypothesis 1 but not hypothesis 2. Province of residence is negatively associated with self-determination
Table 4: The direct effect.
|
Variable |
β |
t |
p-value |
Remarks |
|
Region of origin → Self-determination |
.085 |
1.820 |
.074 |
Supported |
|
Africa |
3.759 |
39.021*** |
.001 |
|
|
America |
.241 |
.958 |
|
|
|
Europe |
-.148 |
-.661 |
|
|
|
Asia |
-.870 |
-2.892** |
.01 |
|
|
Province of residence → Self-determination |
-.012 |
-2.360 |
.022 |
Not Supported |
|
Qinghai |
1.325** |
3.127 |
.01 |
|
|
Shanxi |
.170 |
.581 |
|
|
|
Sichaun |
-.123 |
-.663 |
|
|
|
Zhejiang |
.159 |
.580 |
|
|
|
Hubei |
3.675*** |
24.519 |
.001 |
|
Subsequently, we conduct a hierarchical regression to determine the direct and indirect effects of self-determination on the intention to leave. First, we enter the control variables in Model 1 and include the independent variables in Model 2. In model 3, we introduce the mediator, while in model 4, we include the interaction terms (interaction between the mediator and the independent variables), as shown in Table 5. The composite scale of the independent variables are used to represent the region of origin and province of residence.
We reject hypothesis 3 because the direct effect of region of origin on the intention to leave China is not statistically significant, as shown in model 2. The implication is that the region of origin does not influence the intention to leave China. However, hypothesis 4 is supported because the regression coefficient is positive and statistically significant (β=.014, p<.05), which means that the province of origin influences the intention to leave. As shown in model 3, there is a positive and significant effect on the dependent variable (β=.124*, p<.1). We, therefore, accept the hypothesis that self-determination positively influences the intention to leave, as indicated in hypothesis 5.
For the mediation analysis (indirect effect), we interact the independent variables and the mediator (self-determination) after centering them as recommended by Baron and Kenny (1986) [41]. The results show a statistically nonsignificant effect on the interaction between the region of origin and self-determination (β=-.009, p>.1), based on which we failed to accept hypothesis 6 as shown in model 4. However, the interaction between the province of residence and self-determination has a positive and statistically significant effect on the intention to leave (β=.085, p<.1). There is a 4.1% variance with the addition of the mediator. The indirect effect shows that the higher the infection rate in a province, the more likely an international student will think of leaving China. Hypothesis 7 is, therefore, supported.
Table 5: Hierarchical Regression analysis on the intention to leave China.
|
|
Model 1 |
Model 2 |
Model 3 |
Model 4 |
||||
|
Variable |
Β |
t |
β |
T |
β |
t |
β |
t |
|
Gender |
.081 |
.561 |
-.006 |
-.041 |
-.038 |
-.240 |
.073 |
.439 |
|
Age range |
-.021 |
-.217 |
-.040 |
-.403 |
-.039 |
-.395 |
.095 |
.740 |
|
Level of Education |
-.155* |
-1.772 |
-.016 |
-.120 |
-.022 |
-.164 |
-.045 |
-.334 |
|
Field study |
.122 |
1.529 |
.043 |
.427 |
.030 |
.299 |
.046 |
.445 |
|
Scholarship status |
.108 |
.813 |
-.007 |
-.042 |
-.067 |
-.414 |
.050 |
.295 |
|
Region of origin |
|
|
-.105 |
-1.422 |
-.116 |
-1.558 |
-.037 |
-.103 |
|
Province of residence |
|
|
.014** |
.596 |
.016 |
.660 |
.305* |
-1.798 |
|
Self-determination |
|
|
|
|
.124* |
1.890 |
.401 |
-1.200 |
|
Region of origin*Self-determination |
|
|
|
|
|
|
-.009 |
-.104 |
|
Province of residence*Self-determination |
|
|
|
|
|
|
.085* |
1.912 |
|
R2 |
.098 |
.138 |
.164 |
.231 |
||||
|
∆ R2 |
.098 |
.040 |
.026 |
.067 |
||||
DISCUSSION
The work on SDT repeatedly provides that experiencing self-motivation improves a person’s general well-being and satisfaction (Ryan & Deci, 2017) [16]. In this study, we first tested the effect of the foreigners’ region of origin and province of residence in China on self-determination and the intention to leave China. Also, we established the influence of self-determination on international students’ coping abilities with the outbreak of COVID-19 by their intention to leave China. We further used self-determination to mediate international students’ region of origin and province of residence on the desire to return to their country due to the epidemic/pandemic. The analyzed data showed no effect of region of origin on the intention to return home. However, the province of residence in China greatly influences the intention to return to one’s home country. The reason could be the confirmed infection and death rate in specific provinces and the subsequent evacuation of some foreigners from those provinces. For instance, the Hubei province is called the epicentre of COVID-19 since it was the province of first discovery and high prevalence. As of 14th March 2020, the total number of confirmed cases stood at about 67000, with 3075 fatalities only in the Hubei province (Yin & Xiaoyu, 2020) [43]. China enacted restrictive measures to control the COVID-19 outbreak, including a lockdown of the 12 million residents of Wuhan, which cascaded across the whole of the Hubei province. Other provinces in China subsequently implemented varying levels of restrictive measures, including lockdown, isolation, quarantine, and social distancing. Fear, panic, and restriction on residents will naturally cause anxiety due to measures implemented to curtail the spread of the disease. Also, the incessant media reports on the spread of the virus and its attendant effect increase anxiety and fear. Research has shown that indirect exposure to recurrent media reports of life-threatening events may be enough to generate distress and magnify the risks of common psychological barriers (Neria & Sullivan, 2011)[44]. Furthermore, the unexpected evacuation of nationals of various countries from the Hubei province heightened the desire to leave China. Evidence shows that the inability of other countries to evacuate citizens from Wuhan heightened the anxiety of international students from those countries (Adney, 2020) [45].
The results also show that international students’ level of self-determination influences their desire to return to their home countries to mitigate the fear and anxiety associated with the spread of COVID-19 in China. It shows that the lower the level of self-determination, the more likely the student will nurse plans to leave China. People physically, emotionally, and socially attached to others will find their relationships frustrating in controlled environments (Zhang, Wu, Zhao, & Zhang, 2020) [46]. A series on COVID-19 in the Lancet indicates that quarantining people result in psychological distress, with no signs of abating even after the quarantine (Wang, Horby, Hayden, & Gao, 2020) [47]. Quarantine, isolation, and social distance, when employed, therefore, affect social relationships and physical connection among people. Quarantine and isolation have disrupted people’s jobs and lives immensely and may have important implications for their health, well-being (Liu et al., 2020) [48], and basic psychological needs. This supports the finding that employing strategies such as quarantine and isolation does not support the desire for relatedness.
Similarly, quarantine, even though it may control a pandemic, deprives international students of the desire to experience the warmth and physical support of others or provide support for other foreigners who feel distressed. A shared identity motivates people to be concerned and care for others (Drury, 2018) [49]. Also, physically distancing people conflicts with the human instinct to connect with others (Baumeister & Leary, 1995) [50], particularly during emotional times (Rimé, 2009) [51]. Social connection aids people to manage stress, and remain resilient during difficult times (Jetten et al., 2017) [52]. This is the importance of connectedness, the absence of which increases stress, and produces deleterious effects on the immune system and mental and cardiovascular health (Hawkley & Cacioppo, 2010) [53]. Social distancing, quarantine, and isolation could aggravate the long-term health effects of the COVID-19 epidemic. Even though maintaining contact with others from the home community is essential in psychological adjustment in the new environment (Bektaş, Demir, & Bowden, 2009) [54], Adney (2020) [44], thinks that being prevented from having physical contact for the first time affected the emotional and mental health of students.
Aside from the effect of COVID-19 mitigation strategies on relatedness, autonomy and competence are equally frustrated. Restrictions on movement by city and university authorities result in control rather than autonomy. Students will have to eat at the school canteen rather than having the opportunity to cook their food or eat from their favorite restaurants. The expectation is that international students will follow the strict rules and regulations instituted by authorities, such as reporting to the school coordinator before getting essentials and providing daily updates on one’s health status. Studies show that individuals who experience little autonomy, even in confinement, report a greater sense of well-being and fewer mental health problems (Chua & Koestner, 2008) [55]. Highlighting the autonomous value of being indoors, quarantined or isolated and acknowledging concerns about inconvenience are autonomy-supportive strategies that help individuals internalize the behavior and interpret it as autonomously motivated. Therefore, the level of autonomy experienced even in controlled environments will influence the intention to leave China.
Also, people who experience the need for competence tend to feel effective in their desire to produce accepted outcomes, exhibit their capacities, and build relationships that offer respect and care (Deci & Ryan, 2015)[20]. Competence in crises is critical for making crucial decisions that will have a lasting effect on one’s life. The inability of international students to make decisions without the approval of their school coordinators or undertake an activity they deem necessary without the supervision of others due to restrictions undermines the need for competence. International students knowledgeable in epidemiology or who have read extensively on COVID-19 could offer advice and support to less knowledgeable friends. However, the physical sharing of knowledge through face-to-face activities is not permitted due to the restrictions and controls. International students must contact their school coordinator or specific officials for information, even when such information is sometimes communicated in Chinese and inadequately translated into English. Evidence from Wuhan shows that some international students expressed negative emotions and easily got agitated because of the conflicting and often incomplete information about precautions to take in quarantine due to inadequate communication (Adney, 2020) [44].
Although each basic need contributes uniquely to self-determination, interactively, they are indispensable for people’s well-being across cultures, contexts, and age groups (Kluwer et al., 2020) [32]. Research has shown, and we confirm, that satisfying the three basic needs is critical for wellness, both situationally (Reis et al., 2000) [20] and developmentally (Grolnick et al., 1991) [31]. The satisfaction of the three psychological needs, therefore, results in self-determination.
CONCLUSION
Measures imposed have effectively managed the spread of the virus, with little immediate psychological assistance to the population to help them cope with COVID-19. The absence of such support, coupled with fear-mongering, panic, and the evacuation of foreigners by their respective countries, intensified the effect of the epidemic/pandemic on foreigners. The satisfaction of the basic psychological needs for autonomy, relatedness, and competence is said to function as a fundamental nutrient that energizes the integration process and contributes to the health and psychological well-being. The fulfillment of the three psychological needs results in self-determination, even though each need has a unique effect. Beyond measuring need satisfaction or its absence, needs can be actively thwarted or blocked. Whereas low need fulfillment would fail to foster the growth potential of individuals, the frustration of these needs would elicit defensiveness, ill-being, and even psychopathology (Bartholomew, Ntoumanis, Ryan, Bosch, & Thøgersen-Ntoumani, 2011; Vansteenkiste & Ryan, 2013) [55,56] and in other cases withdrawal. A frustration of the basic psychological needs of international students results in the desire to return to their home countries (Region of Origin).
Basic needs frustration during epidemics is inevitable. Theoretically, we propose that people still have high self-determination if they have the required psychological support to manage epidemics. Therefore, authorities could adopt strategies that support autonomy, competence, and relatedness, as Teixeira et al. (2016) [25]suggested. Additionally, basic psychological needs satisfaction impacts adaptation and crisis management. Practically, we found that the epicenter of an epidemic/pandemic influences the desire of people to flee that area, which is influenced by fear and anxiety, which the containment strategies could exacerbate.
The limited studies on the effect of COVID-19 on uninfected citizens and foreigners limit the discussion since the conditions of previous epidemics are different from what exists on COVID-19. The study of international students’ adaptation to a crisis is also limited; we, therefore, had to juxtapose our analysis with general populations, which may not be appropriate. The reason is that migrants and international students, for that matter, have different sociocultural and economic conditions that make them different from the general population. Hence, research that mainly deals with international students will consider such demographic peculiarity. We also acknowledge the limited sample that prevents the generalization of these findings. We, therefore, suggest a more extensive study in other jurisdictions, such as the United States and Spain, where the confirmed infections of COVID-19 are high.
REFERNCES
-
Houlfort N, Fernet C, Vallerand RJ, Laframboise A, Guay F, Koestner R. (2015). The role of passion for work and need satisfaction in psychological adjustment to retirement. J Vocational Behav. 88:84–94.
-
Philippe FL, Vallerand RJ. (2008). Actual environments do affect motivation and psychological adjustment: A test of self-determination theory in a natural setting. Motivation and Emotion.
-
Vansteenkiste M, Lens W, Soenens B, Luyckx K. (2006). Autonomy and relatedness among Chinese sojourners and applicants: Conflictual or independent predictors of well-being and adjustment? Motivation Emotion. 30(4):273–282.
-
Zhang SX, Wang Y, Rauch A, Wei F. (2020). Health, distress and life satisfaction of people in China one month into the COVID-19 outbreak. MedRxiv.
-
Bitanihirwe BKY. (2016). Monitoring and managing mental health in the wake of Ebola. Annali Dell’Istituto Superiore Di Sanita.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 6736(20):1–10.
-
Clement Addo P, Fang J, Asare AO, Kulbo NB. (2021). Customer engagement and purchase intention in live-streaming digital marketing platforms. Industries J. 1–20.
-
Drosten C, Günther S, Preiser W, van der Werf S, Brodt HR, Becker S, et al. (2003). Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 348(20):1967-1976.
-
Ksiazek TG, Erdman D, Goldsmith CS, Zaki SR, Peret T, Emery S, et al. (2003). A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 348(20):1953-1966.
-
Zaki AM, van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. (2012). Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med. 367(19):1814-1820.
-
WHO. (2004). Summary of probable SARS cases with onset of illness.
-
World Health Organization. (2020a). Coronavirus disease (COVID-19) outbreak.
-
Catalano RF, Berglund ML, Ryan JAM, Lonczak HS, Hawkins JD. (2004). Positive Youth Development in the United States: Research Findings on Evaluations of Positive Youth Development Programs. t Am Acad Pol Soc Sci. 591(1):98–124.
-
Ryan RM. (1995). Psychological Needs and the Facilitation of Integrative Processes. Journal of Personal. 63(3):397–427.
-
Ryan RM, Connell JP. (1989). Perceived locus of causality and internalization: Examining reasons for acting in two domains. J Personal Soc Psychol. 57(5):749–761.
-
Ryan RM, Deci EL. (2017). Self-determination theory: Basic psychological needs in motivation, development, and wellness. New York: Guilford Publications.
-
Deci EL, Ryan RM. (2015). Self-Determination Theory. In: International Encyclopedia of the Social & Behavioral Sciences:486–491.
-
Milyavskaya M, Nadolny D, Koestner R. (2014). Where Do Self-Concordant Goals Come From? The Role of Domain-Specific Psychological Need Satisfaction. Personal Soc Psychol Bulletin.
-
Ng JYY, Ntoumanis N, Thøgersen-Ntoumani C, Deci EL, Ryan RM, Duda JL, et al. (2012). Self-Determination Theory Applied to Health Contexts. Perspectives Psychol Sci: 7(4):325–340.
-
Baard PP. (2004). Intrinsic Need Satisfaction: A Motivational Basis of Performance and Weil-Being in Two Work Settings. J Appl SocPsychol. 34: 2045-2068.
-
Reis HT, Sheldon KM, Gable SL, Roscoe J, Ryan RM. (2000). Daily Well-Being: The Role of Autonomy, Competence, and Relatedness. Personal Soc Psychol Bull. 26(4):419–435.
-
Niemiec CP, Ryan RM. (2009). Autonomy, competence, and relatedness in the classroom. Theory Res Edu. 7(2):133–144.
-
Rigby CS, Ryan RM. (2018). Self-Determination Theory in Human Resource Development: New Directions and Practical Considerations. Adv Dev Human Res. 20(2):133–147.
-
Ryan RM, Deci EL. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 55(1):68–78.
-
Su YL, Reeve J. (2011). A Meta-analysis of the Effectiveness of Intervention Programs Designed to Support Autonomy. Educational Psychology Review.
-
Teixeira PJ, Silva MN, Marques MM. (2016). Identifying self‐determination theory‐ based techniques aimed at promoting autonomy, competence, and relatedness in health contexts. In the Self‐Determination Theory Conference, Victoria; British-Columbia; Canada.
-
Beachboard MR, Beachboard JC, Li W, Adkison SR. (2011). Cohorts and Relatedness: Self-Determination Theory as an Explanation of How Learning Communities Affect Educational Outcomes. Res Higher Edu. 52(8):853–874.
-
Hagger MS, Protogerou C. (2020). Self‐determination Theory and Autonomy Support to Change Healthcare Behavior. In The Wiley Handbook of Healthcare Treatment Engagement, Willey:141–158.
-
Vansteenkiste M, Ryan RM, Soenens B. (2020). Basic psychological need theory: Advancements, critical themes, and future directions. Motivation and Emotion. 44(1):1–31.
-
Ryan RM, Patrick H, Deci E, Williams G. (2008). Facilitating health behaviour change and its maintenance: Interventions based on Self-Determination Theory. European Psychologist.
-
Haerens L, Aelterman N, Vansteenkiste M, Soenens B, Van Petegem S. (2015). Do perceived autonomy-supportive and controlling teaching relate to physical education students’ motivational experiences through unique pathways? Distinguishing between the bright and dark side of motivation. Psychol Sport Exercise.
-
Grolnick WS, Ryan RM, Deci EL. (1991). Inner resources for school achievement: Motivational mediators of children’s perceptions of their parents. J Edu Psychol. 83(4):508–517.
-
Kluwer ES, Karremans JC, Riedijk L, Knee CR. (2020). Autonomy in Relatedness: How Need Fulfillment Interacts in Close Relationships. Personal Soc Psychol Bulletin. 46(4):603–616.
-
Bartholomew KJ, Ntoumanis N, Ryan RM, Bosch JA, Thøgersen-Ntoumani C. (2011). Self-Determination Theory and Diminished Functioning. Pers Soc Psychol Bull. 37(11):1459–1473.
-
Benita M, Benish-Weisman M, Matos L, Torres C. (2020). Integrative and suppressive emotion regulation differentially predict well-being through basic need satisfaction and frustration: A test of three countries. Motivation Emotion. 44(1):67–81.
-
Henning G, Bjälkebring P, Stenling A, Thorvaldsson V, Johansson B, Lindwall M. (2019). Changes in within- and between-person associations between basic psychological need satisfaction and well-being after retirement. J Res Personal. 79:151–160.
-
Mabbe E, Soenens B, Vansteenkiste M, Van Leeuwen K. (2016). Do Personality Traits Moderate Relations Between Psychologically Controlling Parenting and Problem Behavior in Adolescents? J Personal. 84(3):381–392.
-
World Health Organization. (2020b). Coronavirus disease 2019 (COVID-19) Situation Report – 37.
-
Autin KL, Duffy RD, Blustein DL, Gensmer NP, Douglass RP, England JW. (2019). The development and initial validation of need satisfaction scales within the psychology of working theory. J Counseling Psychol. 66(2):195–209.
-
Weisberg J. (1994). Measuring Workers′ Burnout and Intention to Leave. Int J Manpower. 15(1):4–14.
-
Baron RM, Kenny DA. (1986). The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Personality. 51(6):1173–1182.
-
Koslowsky M. (1988). Using Effect Coding For Comparing Models In Social Research. Soc Behav Personal: Int J. (1):85–90.
-
Yin C, Xiaoyu W. (2020). Coronavirus: latest figures show positive trend expanding.
-
Neria Y, Sullivan GM. (2011). Understanding the Mental Health Effects of Indirect Exposure to Mass Trauma Through the Media. JAMA. 306(12):1374.
-
Adney M. (2020). Lessons from ground zero: My COVID-19 lockdown experience in Wuhan.
-
Zhang J, Wu W, Zhao X, Zhang W. (2020). Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: a model of West China Hospital. Precision Clin Med. 3(1):3–8.
-
Wang C, Horby PW, Hayden FG, Gao GF. (2020). A novel coronavirus outbreak of global health concern. Lancet. 395(10223):470–473.
-
Liu S, Yang L, Zhang C, Xiang YT, Liu Z, Hu S, et al. (2020). Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. 7(4):e17–e18.
-
Drury J. (2018). The role of social identity processes in mass emergency behaviour: An integrative review. European Review of Social Psychology.
-
Baumeister RF, Leary MR. (1995). The Need to Belong: Desire for Interpersonal Attachments as a Fundamental Human Motivation. Psychological Bulletin.
-
Rimé B. (2009). Emotion Elicits the Social Sharing of Emotion: Theory and Empirical Review. Emotion Rev. 1(1):60–85.
-
Jetten J, Haslam SA, Cruwys T, Greenaway KH, Haslam C, Steffens NK. (2017). Advancing the social identity approach to health and well-being: Progressing the social cure research agenda. European J Soc Psychol. 47(7):789–802.
-
Hawkley LC, Cacioppo JT. (2010). Loneliness matters: A theoretical and empirical review of consequences and mechanisms. An Behav Med.
-
Bektaş Y, Demir A, Bowden R. (2009). Psychological Adaptation of Turkish Students at U.S. Campuses. Int J Adv Counselling. 31(2):130–143.
-
Chua SN, Koestner R. (2008). A Self-Determination Theory Perspective on the Role of Autonomy in Solitary Behavior. J Soc Psychol. 148(5):645–648.
-
Bartholomew KJ, Ntoumanis N, Mouratidis A, Katartzi E, Thøgersen-Ntoumani C, Vlachopoulos S. (2018). Beware of your teaching style: A school-year long investigation of controlling teaching and student motivational experiences. Learning and Instruction. 53:50–63.
-
Vansteenkiste M, Ryan RM. (2013). On psychological growth and vulnerability: Basic psychological need satisfaction and need frustration as a unifying principle. J Psychother Integr. 23(3):263–280.