2025: Volume 6, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFXanthogranulomatous Cholecystitis Resembling Gallbladder Carcinoma: A Case Report
Mir Arsalan Ali, Amna Soulat, Misha Khan, Umer Shahid*, Muhammad Faez Tahir, Reet Ramani
Ziauddin Medical College, Ziauddin University, Karachi, Pakistan
*Corresponding author: Umer Shahid, Ziauddin Medical College, Ziauddin University, 4/B Shahrah-e-Ghalib Rd, Block 6 Clifton, Karachi, Karachi City, Sindh 75000, Pakistan, Phone: +923353772731, ORCID: 0009-0001-9177-1446, E-mail: [email protected]
Received Date: May 13, 2025
Publication Date: June 13, 2025
Citation: Ali MA, et al. (2025). Xanthogranulomatous Cholecystitis Resembling Gallbladder Carcinoma: A Case Report. Clin Res. 6(1):28.
Copyright: Ali MA, et al. © (2025).
ABSTRACT
Xanthogranulomatous cholecystitis (XGC) represents an uncommon and aggressive manifestation of chronic cholecystitis, showing extensive inflammatory cell involvement of both acute and chronic types. The medical and imaging characteristics of XGC replicate the presentation of gallbladder cancer; therefore, preoperative diagnosis remains challenging. Similar imaging features show up in both chronic illnesses because they both result in gallbladder wall thickening. Histopathologic assessment is vital to diagnosing XGC by examining the presence of xanthoma cells alongside chronic inflammatory cells. Medical experts choose cholecystectomy surgery as the principal therapeutic approach because it involves removing the gallbladder. Preoperative recognition of XGC creates the chance to avoid unnecessary radical surgical operations while producing enhanced outcomes for patients. A middle-aged female patient aged 48 with no existing medical conditions sought medical care for moderate pain in her right upper quadrant along with heart palpitations. Cholecystitis with gallstones appeared on the initial scans and ultrasound examination without signs of cancer emergence. The clinical tests showed liver enzyme abnormalities, indicating cholestasis conditions. The patient underwent cholecystectomy surgery before pathologists confirmed XGC through examination of the resected gallbladder. The imagery of a thickened gallbladder wall requires doctors to include XGC as one of the possible diagnoses for chronic cholecystitis. This report explores more extensively why the diagnosis of XGC depends on accurate pathology tests.
Keywords: Xanthogranulomatous Cholecystitis, Chronic Cholecystitis, Gallbladder Cancer, Gallstone
INTRODUCTION
Xanthogranulomatous cholecystitis (XGC) exists as a rare kind of chronic cholecystitis that manifests through an intense destructive inflammation that attacks the gallbladder wall. Xanthoma cells that contain lipids, which morph into macrophages, appear throughout the gallbladder wall together with dense inflammatory compounds of both acute and chronic cells [1]. The inflammatory process of XGC easily spreads from the gallbladder to adjacent organs, including the liver, duodenum, and colon, which can cause dangerous outcomes, including fistulas, perforations, and abscesses. XGC frequently displays identical radiologic and clinical traits such as gallbladder cancer (GBC); thus, physicians frequently mistake it for malignant disease during preoperative evaluations. An imaging examination usually shows an enlarged gallbladder wall, but this common observation does not provide sufficient evidence to distinguish XGC from cancer. The diagnosis becomes definitive only when a surgeon completes the pathological examination of the removed gallbladder after surgery. XGC shows similar clinical signs to routine cholecystitis, which includes right upper quadrant pain together with cholelithiasis symptoms. These diagnostic difficulties highlight the need for improved preoperative strategies or screening to identify or exclude XGC before surgery. Early and accurate recognition would help avoid confusion with malignancy during surgery and ensure that patients receive appropriate management, ultimately leading to better outcomes.
CASE PRESENTATION
A 48-year-old female, with no known comorbidities, presented to the outpatient department with complaints of moderate right upper quadrant abdominal pain and palpitations for the past 20 days. On further evaluation, it was determined that the palpitations were secondary to dehydration from persistent vomiting, as she had a history of similar episodes of pain along with vomiting and hiccups 20 days back, for which she was admitted to the emergency department and managed conservatively. There was no prior history of cardiac illnesses or risk factors, fever, gastrointestinal bleeding, or weight loss. On physical examination, she was conscious and oriented but mildly dehydrated and hypotensive (BP: 90/60 mmHg). Heart rate was 110 bpm and regular. Abdominal examination revealed tenderness in the right upper quadrant with a positive Murphy’s sign. During the prior admission, an abdominal ultrasound showed a fatty liver with mild hepatomegaly and multiple calculi in the lumen of the gallbladder, one of them measuring 4mm. The common bile duct was of normal caliber, there was no evidence of cholecystitis, and the right kidney showed angiomyolipoma. Importantly, there was no evidence of gallbladder wall thickening, pericholecystic collection, or biliary tree dilation, and no hepatic or pancreatic involvement was noted at that stage. Despite supportive management and intravenous analgesia, the patient continued to experience intense abdominal pain, prompting a non-contrast CT (NCCT) of the abdomen and pelvis to rule out other differential diagnoses such as perforated peptic ulcer, pancreatitis, and renal colic. The NCCT revealed mild gallbladder distention with a maximum wall thickness of 4mm along with fat stranding. No evidence of stone was there to suggest radio-opaque calculi. Her LFTs were also markedly elevated. Given the persistent cholestatic picture and rising bilirubin, endoscopic retrograde cholangiopancreatography (ERCP) was performed and stone extraction 15 days after her first episode of symptoms. The ERCP cholangiogram demonstrated a small filling defect suggestive of stones/sludge. A moderate-sized sphincterotomy was done, followed by balloon sweeping in the gallbladder, and sludge with a small stone was extracted. Post-ERCP baseline labs showed no evidence of infection or any other abnormality. Direct bilirubin and SGPT were within normal limits (direct bilirubin: 0.24 mg/dl, SGPT: 28 IU/l); however, her alkaline phosphatase and gamma GT were high (alkaline phosphatase: 214 U/l, gamma GT: 442 U/l), suggesting a cholestatic picture. Her serum lipase was 167 U/l, slightly higher than the normal limit, not specific for pancreatic involvement. She was scheduled for laparoscopic cholecystectomy after a detailed review and pre-operative fitness.
To further check for malignancy, tumor markers such as CA 19-9 and CEA were considered. However, both were within normal limits, reducing the likelihood of gallbladder carcinoma. Tumor markers are not diagnostic, but they can assist in raising suspicion of malignancy in cases with significant gallbladder wall thickening. Additionally, a contrast-enhanced CT (CECT) of the whole abdomen was considered as a preoperative imaging modality to evaluate local invasion and exclude cancer. CECT provides better delineation of soft tissue planes and can help differentiate inflammatory versus neoplastic processes. However, given the patient's stable condition and ERCP findings, a decision was made to proceed with surgery based on clinical and biochemical assessment.
The patient was non-compliant to surgery when she initially presented in the ER; however, when she presented to OPD after her second attack, which was 21 days after her initial presentation, she underwent surgery within 72 hours of presentation under general anesthesia. A standard four-port laparoscopic technique was used. After creating pneumoperitoneum, Calot's triangle was identified. The cystic duct and artery were independently clipped and separated. Her gallbladder was distinctly inflamed (Figure 1) with thickened walls that were deeply adherent to its bed. Omental adhesions were also appreciated (Figure 2). The gallbladder was then taken out through the umbilical port via a retrieval bag and was sent for histopathological examination. Her port incisions were then closed, and an aseptic dressing was applied. She was extubated in the OR, and her postoperative course was uneventful. Postoperative LFTs showed a declining trend towards normal, and her histopathological report was processed, which showed XGC with evidence of marked surface ulcerations with intact lining. Lamina propria will show moderate to dense infiltration by sheets of foamy histiocytes, eosinophils, lymphoblast cells, and lymphoid aggregates along with a benign reactive lymph node without any evidence of dysplasia or malignancy (Figure 3).
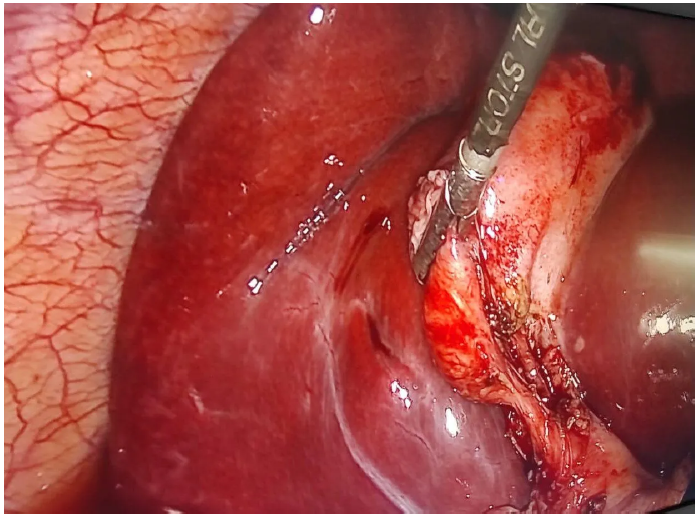
Figure 1. Intraoperative photo showing an inflamed and thickened gallbladder.
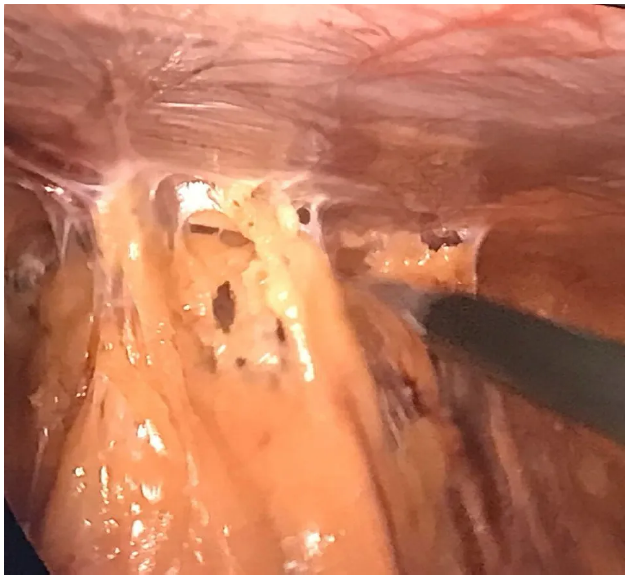
Figure 2. Intraoperative picture showing omental adhesion.
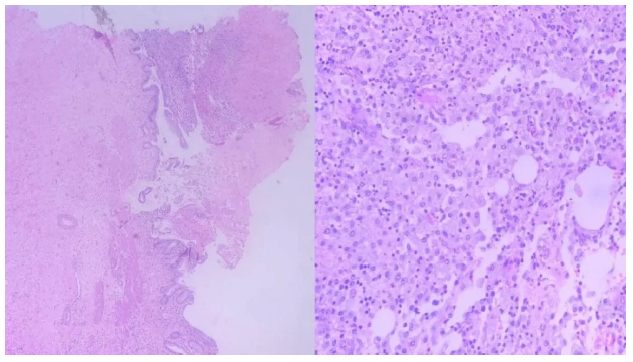
Figure 3. Histological Examination, left picture, low power view of mucosal lining and the right picture; high power view showing sheets of foamy macrophages with Lymphoplasma cell infiltration.
The patient was discharged on the second postoperative day with oral antibiotics and analgesics. The use of antibiotics was integral to her preoperative care, helping to control ongoing inflammation and prevent postoperative infectious complications. She followed up at the OPD a week later, on her eighth postoperative day, for a regular checkup and had no active complaints; her incision sites showed healing. Although a follow-up abdominal ultrasound was performed, which showed no evidence of pancreatic involvement or any visceral abnormality, it is recognized that ultrasound has limited sensitivity in detecting subtle pancreatic or deep visceral complications. Therefore, a CECT of the abdomen was also performed postoperatively, which showed no evidence of pancreatic involvement or other intra-abdominal abnormalities. The patient was advised to follow up in OPD every three months if no symptoms develop.
DISCUSSION
XGC is a rare inflammatory manifestation of the gallbladder, ranging from 1.9% in Europe and the USA [2], first described in the literature in the 1970s [3]. It is marked by acute and chronic inflammatory cell infiltration and intramural lipid-laden macrophage accumulation [4]. Grossly, it appears as yellow-gray nodules called xanthogranuloma or xanthoma (foamy histiocytes containing lipids and bile pigments) [1], and it usually spreads to involve nearby structures, which is why it was previously coined as ‘benign gallbladder pseudotumor.’ There is no gender or age predominance seen in cases of XGC, but it usually occurs at an average age of 49 to 62 [5]. Clinical symptoms of XGC are nonspecific and like those of acute or chronic cholecystitis. Its aggressive characteristics include fistula, abscess, perforation, and invasion of nearby organs. Intraoperative frozen segment analysis or postoperative histopathological examinations are usually the most common means to diagnose it, as it is generally misunderstood as GBC due to similar wall thickening characteristics. The goal of imaging is to establish a connection between focal or diffuse gallbladder wall thickening and to rule out the diagnosis of GBC to prevent the patient from receiving inappropriate management and to avoid an unwarranted extensive resection for what is a benign condition. The addition of diffusion-weighted imaging to conventional MRI improves discrimination between XGC and the wall-thickening type of GBC [6].
While imaging findings often overlap between XGC and gallbladder carcinoma, adjunct investigations such as tumor markers (CA 19-9, CEA) and preoperative CECT can support clinical decision-making. Elevated CA 19-9 is occasionally reported in XGC but may also indicate malignancy, thus lacking specificity. Preoperative CECT is especially valuable when malignancy cannot be excluded on USG or initial CT, as it helps evaluate lymph node status, hepatic infiltration, and nearby structures, guiding the extent of surgical intervention.
Another diagnostic approach that is still under discussion is endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) cytology of the gallbladder. In a cohort study, XGC was suspected in 6 out of 15 individuals; cytology revealed that 3 patients showed foam cells, 1 showed inflammatory cells, 1 showed GBC, and 1 sample was insufficient but was later diagnosed to be XGC [7]. This study concluded that malignant GB mass lesions can be safely and accurately differentiated by EUS-FNA; thus, patients with XGC can avoid undue extensive surgery. Although not specific, an inflammatory condition characterized by high WBC and CRP and elevated transaminases is frequently observed. It is possible to observe cholestasis with increased conjugated bilirubin, especially in the presence of choledocholithiasis [6]. The histopathological findings usually represent xanthoma cells, enormous multinucleated histiocytes, and diffuse or focal mural alterations. These histiocytes exhibit CD68 immunohistochemical positivity. The gallbladder wall also frequently experiences microabscesses, which ultimately lead to a fibrous reaction and scarring as the inflammatory reaction heals. The gallbladder's serosal lining ruptures, and the inflammatory response spreads, causing adhesions to form with the neighboring duodenum, liver, and transverse colon. Ultrasound findings correspond with the presence of gallstones or sludge along with wall thickening [1].
To distinguish XGC from GBC preoperatively is still a challenge, and due to its invasive nature, surgical treatment seems to be the management of choice. About 30% of XGC patients experience challenges like gallbladder perforation, bile duct blockage, liver abscesses, and fistulas to the stomach, duodenum, or liver. Because of the significant fibrotic and inflammatory nature of XGC, open cholecystectomy is frequently necessary. The laparoscopic technique, however, should be tried first because the conversion rate ranges from 10% to 80%. The laparoscopic approach is associated with more intraoperative complications, such as bile duct injury and bile fistula [2,8], which can lead to bilioperitoneum, causing surgical site infection, liver abscess, and bleeding [6,9].
In addition to sharing certain similarities with carcinoma, XGC appears to be positively associated with the development of cancerous tumors. It's unclear why there is this link. It might just be the case that adenocarcinoma and XGC are both consequences of cholelithiasis and cholecystitis of a specific length or severity, or it might be the case that tissue disruption caused by cancer makes it easier for bile to enter the stroma, thus requiring a proper preoperative diagnosis and management [10]. In any case of XGC, thorough sectioning of the gallbladder (and any suspicious areas) is required to exclude an occult carcinoma. Likewise, if there is any intraoperative suspicion of malignancy, frozen section analysis and an oncological surgical approach are warranted.
CONCLUSION
XGC is an uncommon, benign inflammatory condition that closely mimics gallbladder carcinoma. Early recognition is essential to avoid unnecessary aggressive surgery and manage intraoperative challenges associated with dense adhesions; for example, ultrasound-guided fine-needle aspiration cytology (FNAC) of the gallbladder wall or frozen section biopsy of the gallbladder can be done to rule out any malignancy of the gallbladder and unnecessary resection of the liver. Histopathological confirmation remains crucial for definitive diagnosis and appropriate patient care.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was not required for this case report by the institutional policies. Written informed consent was obtained from the patient for participation in and publication of the study.
CONSENT FOR PUBLICATION AND ANY ACCOMPANYING DATA
Written informed consent was obtained from the patient for publication of this case report.
AVAILABILITY OF DATA AND MATERIALS
This manuscript does not report data generation or analysis.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
The authors received no specific funding for this work.
AUTHORS’ CONTRIBUTIONS
Mir Arsalan Ali, Amna Soulat, and Misha Khan have given substantial contributions to the conception or the design of the manuscript, Umer Shahid, Muhammad Faez Tahir, and Reet Ramani to acquisition, analysis, and interpretation of the data. All authors have participated in drafting the manuscript, and Misha Khan has revised it critically. All authors read and approved the final version of the manuscript.
REFERENCES
- Singh VP, Rajesh S, Bihari C, Desai SN, Pargewar SS, Arora A. (2016). Xanthogranulomatous cholecystitis: What every radiologist should know. World J Radiol. 8(2):183-191.
- Frountzas M, Schizas D, Liatsou E, Economopoulos KP, Nikolaou C, Apostolou KG, et al. (2021). Presentation and surgical management of xanthogranulomatous cholecystitis. Hepatobiliary Pancreat Dis Int. 20(2):117-127.
- Christensen AH, Ishak KG. (1970). Benign tumors and pseudotumors of the gallbladder. Report of 180 cases. Arch Pathol. 90(5):423-432.
- Chauhan SS, Kumar N, Rana F. (2023). Xanthogranulomatous Cholecystitis Mimicking Gall Bladder Cancer: a Diagnostic Dilemma and Review of Literature. Indian J Surg Oncol. 14(4):796-799.
- Giudicelli X, Rode A, Bancel B, Nguyen AT, Mabrut JY. (2021). Xanthogranulomatous cholecystitis: Diagnosis and management. J Visc Surg. 158(4):326-336.
- Kang TW, Kim SH, Park HJ, Lim S, Jang KM, Choi D, et al. (2013). Differentiating xanthogranulomatous cholecystitis from wall-thickening type of gallbladder cancer: added value of diffusion-weighted MRI. Clin Radiol. 68(10):992-1001.
- Hijioka S, Mekky MA, Bhatia V, Sawaki A, Mizuno N, Hara K, et al. (2010). Can EUS-guided FNA distinguish between gallbladder cancer and xanthogranulomatous cholecystitis? Gastrointest Endosc. 72(3):622-627.
- Ayadi TY, Behi H, Guelmami H, Changuel A, Tlili K, Khalifa MB. (2024). Xanthogranulomatous cholecystitis: Diagnostic dilemma and surgical solution in geriatric patients: A case report. Int J Surg Case Rep. 120:109857.
- Khan S, Abeer I, Husain M, Hassan MJ, Jetley S. (2021). Xanthogranulomatous cholecystitis mimicking advanced gallbladder carcinoma - Analysis of 8 cases. J Cancer Res Ther. 17(4):969-975.
- Benbow EW. (1989). Xanthogranulomatous cholecystitis associated with carcinoma of the gallbladder. Postgrad Med J. 65(766):528-531.